

Practice Perfect 895
Fifth Metatarsal Base Fractures:
Understand Them for Proper Treatment
Fifth Metatarsal Base Fractures:
Understand Them for Proper Treatment

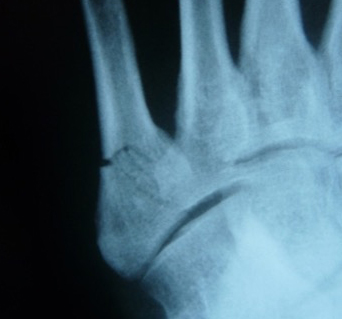
The 2024 CASPR/NMS residency interviews are complete. It was a long weekend - much longer, I'm sure, for those interviewing. Every year it seems there's one topic that surprises me that many students answer incorrectly. Previously, biomechanics topics were the most missed. This year, it was fifth metatarsal base fractures. Over and over again, I witnessed students misdiagnose and recommend the wrong treatment for the wrong reasons for a relatively simple case of a nondisplaced fifth metatarsal avulsion fracture (see Figure 1).

Want to avoid misdiagnosing and applying the wrong treatment for the wrong reasons for a relatively simple case of a nondisplaced fifth metatarsal avulsion fracture?
Read on...
Since this fracture was so commonly misidentified and mistreated, let's review this topic and see if we can clarify the thought process for proper treatment. One simply needs to understand two things: anatomy and mechanism of these fractures.




Anatomy
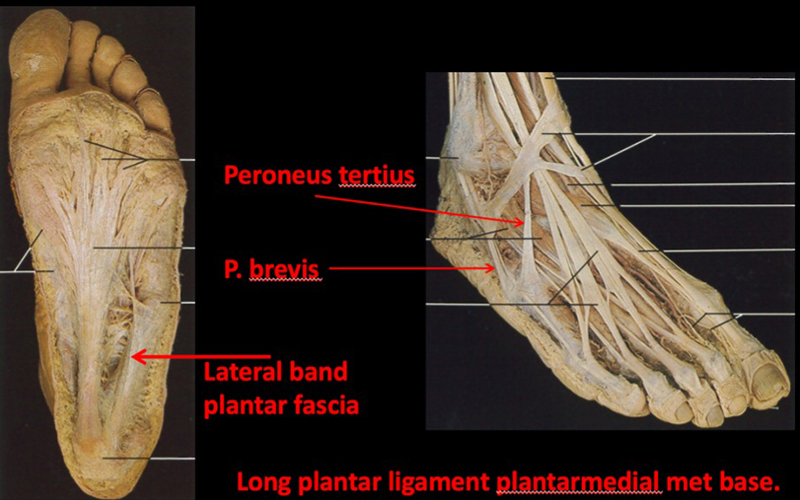
Obviously, there's a lot of detail to anatomy, but we can boil down the most important aspects to two things: attachments to the fifth metatarsal base and blood supply. You can see in Figure 21 the primary ligamentous and tendinous attachments to the bone, creating a strong and stable base. Note two tendons attach directly to the base and that there are less attachments distal to the base, allowing for greater mobility, especially at the shaft.
Blood Supply
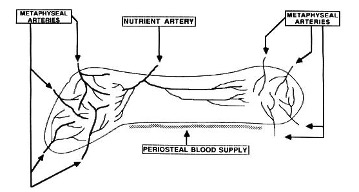
Next, note in Figure 32 the arterial distribution to the bone. The base and head aspects have a larger and more random supply of flow, allowing continued vascular supply in case of a fracture, while the shaft is supplied by only one nutrient artery, leaving a more diminutive vascularization. If a trauma occurred, damaging this supply, there's a much greater chance of interrupting the flow to the bone at this "watershed" area. These two concepts together explain much of the why fractures occur in the pattern they do and why certain fractures demand surgery while another allows nonsurgical treatment.
Putting It Together
Knowing this information and considering the mechanism of the common fractures allows us to determine proper treatment. There are three primary types of fractures: avulsion, Jones, and stress fractures. Because Jones and stress fractures occur within the watershed shaft area and are generally treated the same, let's lump them together. There are now only two base fractures to worry about: avulsion and Jones/stress.
Avulsion Fractures
Remembering the ligamentous and tendinous anatomy, we can easily understand that an inversion of the ankle will create increased tension on the attached ligaments, while the peroneus brevis and tertius muscles actively fire while attempting to stabilize the ankle. These structures pull on the bone, rapidly yanking off a piece of the metatarsal base. Because of their specific locations of attachment, we see the classic straight transverse fracture at the base, typically proximal to the fourth-fifth metatarsal articulation, as shown in Figure 1. Remember, avulsion fractures tend to be transverse right at the location of tendon and ligament attachments. Recall also that this location is well vascularized with that random blood flow, leading to a high rate of fracture healing. There is reasonable research evidence that these fractures do NOT require surgery and are successfully treated with immobilization3,4,5.
Remember, avulsion fractures tend to be transverse right at the location of tendon and ligament attachments. There is reasonable research evidence that these fractures do NOT require surgery and are successfully treated with immobilization
Jones/Stress Fractures
The same anatomical knowledge can help us understand and properly treat these fractures as well. Anatomically, they are located around the border zone of a very stable base and a potentially moveable shaft. This same area, in an evolutionarily unfortunate twist of fate, is the one with a decreased and more delicate vascular supply. Kavanaugh, et al showed that Jones fractures occur due to a combination of vertical forces (pushing upwards on the plantar foot) and mediolateral forces combined with a failure of the foot (to) invert during a walking injury (the opposite of the avulsion fractures). The base remains stable, and the avascular area becomes the hinge of the fracture. Varus hindfoot position has also been implicated7, and I've seen a good number of these in patients with metatarsus adductus and pes cavus. It's the "up down/side to side" motion at an area of weakness with an easily disrupted blood supply that creates this fracture and greatly increases the risk of nonunion. It's this nonunion risk that dictates the need for surgery. In no less than seven studies, the risk of nonunion was greater in patients treated non-surgically, and the overall outcomes were much better in patients treated surgically3,6,8,9,10,11,12.
It's the "up down/side to side" motion at an area of weakness with an easily disrupted blood supply that creates Jones/Stress fractures and greatly increases the risk of nonunion. It's this nonunion risk that dictates the need for surgery. In no less than seven studies, the risk of nonunion was greater in patients treated non-surgically, and the overall outcomes were much better in patients treated surgically
The reason stress fractures are treated the same as Jones fractures is because of the location rather than the mechanism. A slower prodrome rather than an acute injury differentiates these two fractures that look the same on radiographs. In my mind, a stress fracture requires an additional investigation into other causes of bone weakness such as vitamin D deficiency and osteoporosis along with a careful biomechanical examination.




Wrapping It Up!
Now, one may ask, do I stick to these rules rigidly? Of course, not! Every patient is unique and should be considered that way. Displaced fractures may need surgery, regardless of their location. Similarly, atypical or comminuted fractures might need stabilization. Similarly, I've treated patients with Jones fractures non-surgically. Not everyone is a surgical candidate! In patients like this with Jones or stress fractures, I tend to cast them initially but schedule a closer follow-up with serial radiographs. If I see concerning signs (sclerosis, complete lack of trabeculation, or fracture enlargement on radiographs), then I'll plan for surgery.
Keeping in mind these logical and not overly complex factors, one can make sound decisions, maintaining successful outcomes. Remember, students, although the interviews are over, there's still four months of school left. This is the time to increase your studying to be ready for residency. Good luck in the match and best wishes!
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]
- Rohen J, Yokochi C, Lutjen-Drecoll E Color Atlas of Anatomy. 4th ed 1998.
Follow this link
- Smith JW, Arnoczky SP, Hersh A. The interosseous blood supply of the fifth metatarsal: implication for proximal fracture healing. Foot Ankle. 1992 Mar-Apr;13(3):143-152.
Follow this link
- Clapper MF, O'Brien TJ, Lyons PM. Fractures of the fifth metatarsal. Analysis of a fracture registry. Clin Orthop Relat Res. June 1995;315:238-241.
Follow this link
- Weiner BD, Linder JF, Giattini JF. Treatment of fractures of the fifth metatarsal: a prospective study. Foot Ankle Int. 1997 May;18(5):267-269.
Follow this link
- Egol K, Walsh M, Rosenblatt K, Capla E, Koval KJ. Avulsion fractures of the fifth metatarsal base: a prospective outcome study. Foot Ankle Int. May;28(5):581-583.
Follow this link
- Kavanaugh JH, Brower TD, Mann RV. The Jones fracture revisited. J Bone Joint Surg Am. 1978 Sep;60(6):776-782.
Follow this link
- Raikin SM, Slenker N, Ratigan B. The association of a varus hindfoot and fracture of the fifth metatarsal metaphyseal - diaphyseal junction: the Jones fracture. Am J Sports Med. 2008 Jul;36(7): 1367-1372.
Follow this link
- Mologne T, Lundeen JM, Clapper MF, O'Brien TJ. Early screw fixation versus casting in the treatment of acute Jones fractures. Am J Sports Med. 2005 Jul;33(7):970-975.
Follow this link
- Dameron Jr TB. Fractures and anatomical deviations of the proximal portion of the fifth metatarsal. J Bone Joint Surg Am. 1975 Sep;57(6):788-792.
Follow this link
- Josefsson PO, Karlsson M, Redlund-Johnell I, Wendeberg B. Jones fracture. Surgical versus nonsurgical treatment. Clin Orthop Relat Res. 1994 Feb;(299):252-255.
Follow this link
- Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M. Fractures of the base of the fifth metatarsal distal to the tuberosity. Classification and guidelines for non-surgical and surgical management. J Bone Joint Surg Am. 1984 Feb;66(2):209-214.
Follow this link
- Fernandez Fairen M, Guillen J, Busto JM, Roura J. Fractures of the fifth metatarsal in basketball players. Knee Surg Sports Traumatol Arthrosc. 1999;7(6):373-377.
Follow this link




















Comments
There are 0 comments for this article