

Practice Perfect 850
Giving Feedback
Giving Feedback

One of the most important aspects of teaching anyone, whether student, resident, or even a physician in practice, is providing feedback. Unfortunately, this is perhaps the most challenging aspect of teaching.
I see several barriers to feedback of which we should be aware. First, is the Charlie Brown effect. Remember how all of the adults in the Peanuts TV series made that mumbling “wah wah wah” sound while speaking? This, of course, implied that what the adults had to say was unimportant and not worth knowing (obviously wrong). I see the Charlie Brown effect in students who are either overwhelmed by what they’re hearing or do not accept what they’re hearing. I’ve also seen this happen when the feedback provided goes on for an excessively long period of time.
Second is the screeching sound a microphone makes when picking up the sound from its speaker while the speaker is playing the sound from the microphone. It's apropos, and not a little ironic, that this is called feedback. We have all heard this horrible noise. When working with trainees, I imagine they hear this sound when I or one of my academic partners gives them negative feedback or uses overly "creative" wording to describe their errors.
Third, and most unfortunate, is the deer-in-the-headlights appearance of a trainee simply petrified in fear by their attending. I've seen that look in many a trainee's eyes, especially when working with attendings that intimidate trainees. Sometimes being so intimidated by a person makes one unreceptive to what the preceptor is saying.




Despite these barriers, good feedback is highly effective. What can we, as teachers, do to improve our feedback and make it more effective? This is easier said than done. Because of the nature of our hierarchical relationship with trainees, we may often see the deer-in-the-headlights look, limiting the effectiveness of our feedback. The only way to decrease this is to create an open and safe environment. Make sure you verbalize and demonstrate that trainees will not be berated, made fun of, or embarrassed during their time with you. It should also be clear that learning only occurs when we search out and recognize mistakes and areas of deficiency. When a trainee sees that a mistake is received by you in a good-natured way, they will feel a little less tentative.
One of the ways to do this is to avoid being overly descriptive about their mistakes. For example, picture yourself as the attending physician listening to a case presentation about a new patient with heel pain.
"What is your differential diagnosis?" you ask the student.
"I think it's plantar fasciitis," he responds.
"Can you think of other differentials?" you push back.
"Ugh," the student pauses thinking. "A foreign body?" he says.
"That's the worst differential diagnosis I've ever heard. Where did you go to school, and did you even bother studying?" you gripe angrily, proceeding to list off every differential known to humanity.
In this situation, I can hear that screeching microphone sound, see the deer-in-the-headlights, and imagine the Charlie Brown effect occurring. As much as you want the student to understand your frustration with their below-expectations performance, this is unlikely to elicit any productive learning on their part. It serves to embarrass the student, and the information you provide is likely too much for them to retain. Instead, take a breath, do not chastise the student, but rather focus on the details of what they did wrong and impart only one or two learning points. You might suggest, for example, for the student to state differentials of heel pain by the anatomy of the area, then give the student some homework to read about the differential diagnosis of heel pain and report back to you tomorrow.
If it turns out that this lack of knowledge represents a larger issue (ie, that their performance is below their peers) then a separate conversation at another time, away from others, in an unhurried environment is necessary. This gives the preceptor a chance to phrase their concerns in a proper way, asking the learner what they think of the problem and provide suggestions to improve.
One of my colleagues at WesternU does a fantastic job framing student problems before giving the actual feedback. First, she always finds something positive to say. For example, “That’s a good start to the differential diagnosis of heel pain...” This is said without raising her voice or adding in a tone of judgement. She then categorizes the error. “…but there is a larger differential that is important.” No judgement or chastising necessary. The student is made aware of a deficiency in a safe way without feeling embarrassed.
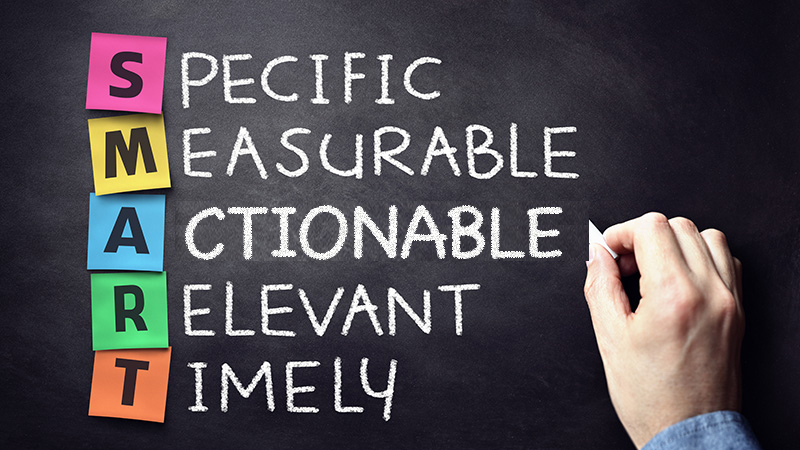
We are not all masters at giving feedback, so having a framework can sometimes be helpful. The acronym SMART has been used in many arenas, and, also works here. Your feedback to trainees should be SMART:
- Specific - make it clear exactly what they did wrong or right.
- Measurable - consider asking for a presentation they should create to prove that they learned.
- Actionable - vague comments do not allow for improvement of a skill. Focus on an item on which they can improve.
- Relevant - the focus should be on what is important to the learner since adults learn better when the context is pertinent to them.
- Timely - do not wait too long to provide feedback or that feedback may never happen.
I would argue that the most important of these is the specificity of a preceptor’s feedback. Being vague provides nothing useful for the trainee to focus on to improve. The most common feedback my residents receive from their attendings during performance reviews is the statement, “A pleasure to work with. Doing a great job.” As much as I like knowing the residents are succeeding at their rotations, it’s not possible that they did a perfect job and had something they could have improved on. Making that feedback more specific helps the learner understand exactly what they need to work on to improve.




In summary, our feedback should exist in a safe environment, be as specific as possible, be given at the right time, in a manner that gives our learners something to focus on and provides the opportunity to follow-up and prove that they learned. None of us are perfect (I’ve made more mistakes teaching than I can count!), and we all lose opportunities to help our trainees grow and learn, but a few simple rules will help guide each of us to being better preceptors and make our trainees more successful.
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]

Major Sponsor





















Comments
There are 0 comments for this article