

Paths to Practice Perfection
Measurement of Tissue Oxygenation and Temperature in Wounds Treated with TWO2 Therapy
Measurement of Tissue Oxygenation and Temperature in Wounds Treated with TWO2 Therapy

Matthew Regulski, DPM,
FFPM RCPS (Glasg), ABMSP, FASPM
Medical Director
The Wound Care Institute of Ocean County, NJ
Senior Partner
Ocean County Foot and Ankle Surgical Associates
Toms River, NJ
This case series involves patients with chronic ulcers to assess healing of their wounds treated with TWO2 therapy using a multispectral near-infrared spectroscopy (NIRS) imaging device to measure tissue oxygenation (StO2) and temperature.
TWO2 therapy has been shown to increase tissue oxygenation and sustain it over time, resulting in reduced infection, improved angiogenesis, and the formation of higher tensile strength collagen during wound healing1–3. Cyclical pressurized topical oxygen (TWO2) therapy combines high concentration oxygen delivery with therapeutic level cyclical compression, which reduces edema, improves wound bed perfusion, and allows more efficient oxygen diffusion, nutrient exchange, and removal of inflammatory factors. Both patients self-administered TWO2 therapy, 5 days a week, 90 minutes per session, within the comfort of their own homes.
Patient 1
A 55-year-old male smoker, with a left lateral diabetic foot ulcer, present for 3 months.
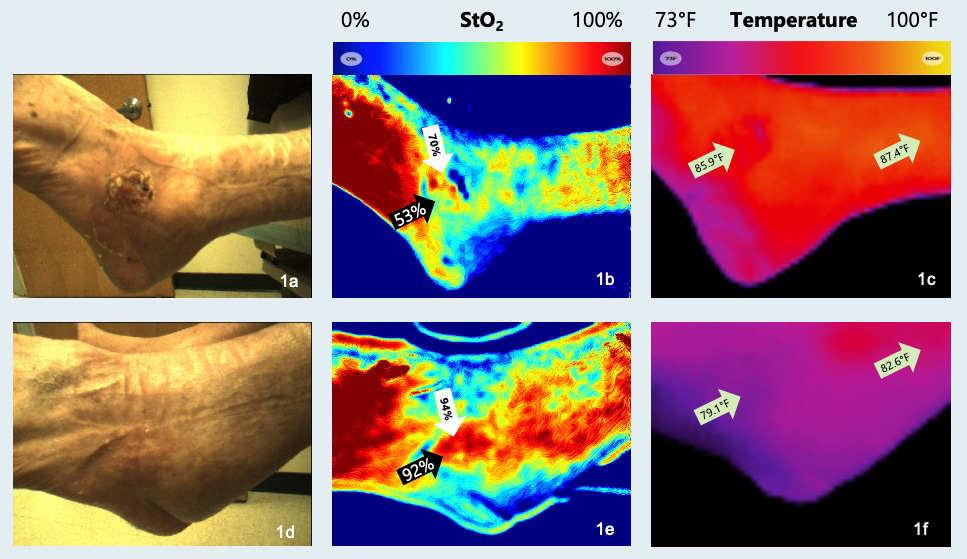
Figures 1a-1c: Start of TWO2 therapy and NIRS imaging. Figure 1c: No increase in temperature within wound compared to control site. Note: Reviewing the visual images of wound bed oxygenation with the patient convinced him to try to stop smoking. Figures 1d-1f: Week 5. Figure 1d: Wound closed. Figure 1e: Black arrow - 39% increase in StO2. White arrow - 24% increase in StO2 (tissue oxygenation within wound bed). Figure 1f: No increase in temperature within wound compared to control site.
Patient 2
A 76-year-old female, with a five-year history of recurrent right, medial ankle ulceration, complicated by lupus, chronic venous insufficiency and treated with radiation therapy for skin cancer. Prior to initiation of TWO2 therapy patients had been treated with standard of care for at least two months, including debridement, edema management, moist wound dressings, and appropriate medical management, with little wound improvement. TWO2 therapy was initiated one year prior to the imaging shown in Figures 2a-2c, and her wound volume had decreased by 95% during that time. Her wound at the start of TWO2 treatment is shown in Figure 2a.

NIRS imaging depicts the final 12 weeks of healing.
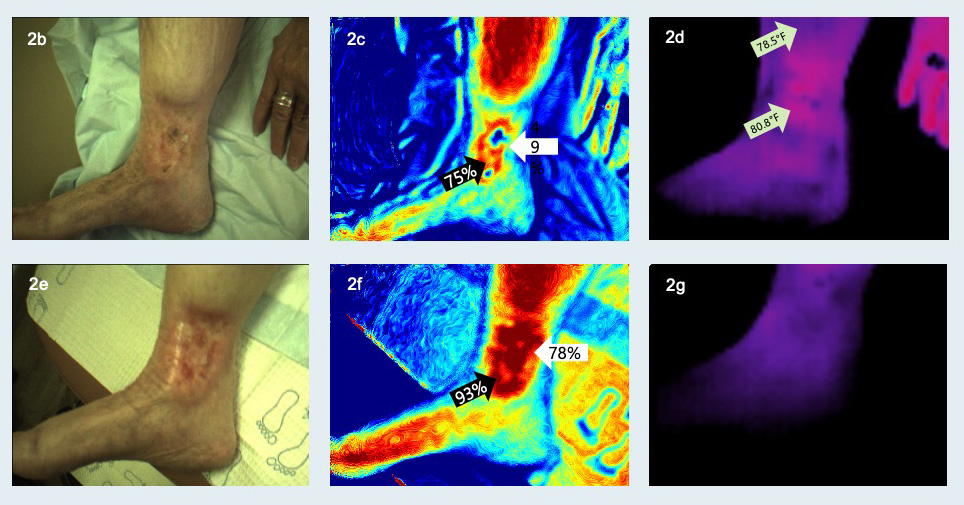
Figures 2b-2d: Start of NIRS imaging. Figure 2d: Thermal image shows 2.3°F (1.3°C) increase in wound bed compared to control site. Possible sign of inflammation. Figures 2e-2g: Week 12 of NIRS imaging. Figure 2e: Wound closed. Figure 2f: Black arrow - 18% increase in StO2. White arrow - 29% increase in StO2. Figure 2g: Thermal imaging of wound bed is cut-off.
Conclusion
NIRS data provided objective measures of increases in StO2, allowing for quantitative assessment of oxygen delivery to the tissue. Using NIRS data, it is clear that using TWO2 therapy, via pressurized oxygen delivery, can lead to a dynamic increase in oxygen saturation levels as measured by StO2. As a result of this rapid increase in oxygen saturation, the wound healing sequence, as we understand it, was able to accelerate in function, as the wound healing environment continued to improve4. This allowed for rapid angiogenesis and new capillary bed formation. TWO2 therapy was effective in decreasing pain, via improving wound bed vascularity and achieving significant wound size reduction. This was demonstrated in two medically complex patients with a late-effect soft tissue radiation injury, and chronic ulcer that were refractory to standard of care and had few other options for treatment.
Do you have questions regarding TWO2 Therapy?
Connect with AOTI
As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
NOTE: Specific indications, contraindications, warnings, precautions, and safety information exist for this product and therapies. Please consult a clinician and product instructions for use prior to application. Rx only.
-
Gordillo GM, Sen CK. Evidence-Based Recommendations for the Use of Topical Oxygen Therapy in the Treatment of Lower Extremity Wounds. doi:10.1177/1534734609335149
Follow this link -
Gordillo GM, Roy S, Khanna S, et al. Topical oxygen therapy induces vascular endothelial growth factor expression and improves closure of clinically presented chronic wounds. doi:10.1111/j.1440-1681.2008.04934.x
Follow this link -
Fries RB, Wallace WA, Roy S, et al. Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat Res. 2005 Nov 11;579(1-2):172-181.
Follow this link -
Sen CK. Wound healing essentials: let there be oxygen. Wound Repair Regen. 2009 Jan-Feb;17(1):1-18. doi: 10.1111/j.1524-475X.2008.00436.x. PMID: 19152646; PMCID: PMC2704021.
Follow this link

Comments
There are 0 comments for this article