

Practice Perfect 928
Why I Like the Lapidus Bunionectomy
Why I Like the Lapidus Bunionectomy


In podiatric surgery, the bunionectomy is one of the most common surgical procedures that we do. Interestingly, hallux valus is one of the very complex deformities that we do not fully understand, even now after years of research and treatment. With that in mind, it is not surprising that there are so many surgical procedures available to repair hallux valgus deformities. For me, like an increasing number of surgeons, my preferred bunionectomy procedure is the Lapidus. I would like to take the rest of this editorial to explain why I prefer this procedure.
Before I do that, though, I want to state the disclaimer at the outset that this is not the only procedure that I do. I do not cookbook my surgeries but rather attempt to thoughtfully choose what I think will be best in discussion with each patient. Also, I do not have a particular recommendation for fixation or different versions of the procedure, so I am not advertising a particular product. This discussion is more about the procedure itself. With that said, let's get to it.

Correction at the Apex
When I was trained to perform metatarsal osteotomies, especially metatarsal head osteotomies, it became clear very quickly that we were taking what looked like a normal bone in a wrong position and cutting that bone to create an abnormal bone in a better position. When performing the Lapidus procedure we are focusing the surgery on the apex of the deformity or the CORA (center of rotational angulation). This satisfied the first CORA principle well.


Figure 1. Lapidus bunionectomy with postoperative radiograph demonstrating correction at the deformity and anatomical alignment of the sesamoids.



Several biomechanical cadaver studies have shown well that sagittal plane movement of the medial column of the foot occurs differentially at each of the three joints1,2,3(Figure 2). As a general conclusion from these studies, it is near 50% of the motion at the naviculocuneiform joint and the first tarsometatarsal joint, with a much smaller contribution of the talonavicular joint. As a quick side note, transverse plane movement of the foot is dominated by the talonavicular joint. As a result, this procedure additionally reduces or stabilizes the arch. As we all know, part of the complex ideology of bunions involves instability to some degree of the medial arch.
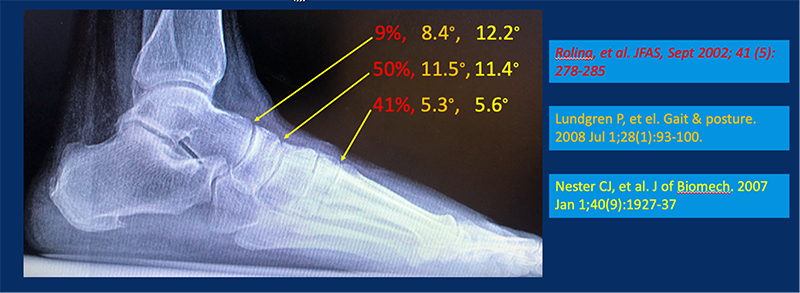
Figure 2. Three studies demonstrating the multi-joint involvement of sagittal plane motion of the medial longitudinal arch. Colors indicate the amount of joint motion found during each study.
The additional benefit of this procedure is also evident from the biomechanical research from Perez, et al4, Johnson and Christensen5, and Bierman, et al6. Perez, et al found that rotating the first metatarsal into a relative valgus position created a close-packed position of the first tarsometatarsal joint, improving stability, while Johnson and Christensen’s classic study (part of their excellent five-part biomechanical cadaver series) characterized the important role of the peroneus longus tendon on increasing arch stability. Bierman and colleagues then showed that fusion of the first tarsometatarsal joint stabilized the medial column. The take-away from these studies is the power of the Lapidus procedure to not only realign deformity at the first MTP joint but also to improve overall foot function. That’s a powerful procedure!
I can’t help but to insert one more study from that classic series of five from Dr Christensen’s group. Rush, et al found that when the sesamoids were properly aligned plantar to the first metatarsal head, the windlass mechanism of the foot was more effective. Yet another functional benefit! There’s also some early evidence that proper sesamoid alignment after bunionectomy leads to decreased recurrence. As a result of this, I aim for this anatomical alignment whenever performing bunionectomies (regardless of the type).
Because of these strong biomechanical effects, the Lapidus bunionectomy has become my procedure of choice for hallux valgus correction.
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]
- Roling BA, Chistensen JC, Johnson CH. Biomechanics of the first ray. Part IV: The effect of selected medial column arthrodesis. A three-dimensional kinematic analysis in a cadaver model. J Foot Ankle Surg. 2002 Sep-Oct;41(5):278-285.
Follow this link
- Lundgren P, Nestor C, Liu A, et el. Invasive in vivo measurement of rear-, mid- and forefoot motion during walking. Gait Posture. 2008 Jul;28(1):93-100.
Follow this link
- Nester CJ, Liu AM, Ward E, et al. In vitro study of foot kinematics using a dynamic walking cadaver model. J Biomech. 2007;40(9):1927-1937.
Follow this link
- Perez HR, Reber LK, Christensen JC. The effect of frontal plane position on first ray motion: forefoot locking mechanism. Foot Ankle Int. 2008 Jan;29(1):72-76.
Follow this link
- Johnson CH, Christensen JC. Biomechanics of the first ray. Part 1. The effects of peroneous longus function: a three-dimensional kinematic study on a cadaver model. J Foot Ankle Surg. 1999 Sep-Oct;38(5):313-321.
Follow this link
- Bierman RA, Christensen JC, Johnson CH. Biomechanics of the first ray. Part III. Consequences of Lapidus arthrodesis on peroneus longus function: a three-dimensional kinematic analysis in a cadaver model. J Foot Ankle Surg. 2001 May-Jun;40(3):125–131.
Follow this link

Overall sponsorship of PRESENT Podiatry was
made possible through the support of our sponsors:


















Comments
There are 0 comments for this article