

Practice Perfect 889
Things We Do for No Reason: Overnight Vital Signs
Things We Do for No Reason: Overnight Vital Signs


As a proponent of logic and reason in the care of our patients, I greatly appreciate when something is brought to my attention that makes me ask, “Why do we do that?” As such, I love the ongoing series called CHOOSING WISELY®: THINGS WE DO FOR NO REASON™ published by the Journal of Hospital Medicine. If you haven’t seen this, I strongly recommend taking a look. Most of it relates to general medicine topics, but some of the topics also relate to podiatry.



Let’s take a look at and amplify one of the topics from this important series. Given the work many podiatrists do in hospitals, we often come across patients who are exhausted both from their disease and from being constantly awakened for nurse checks, blood draws, rounds, beeping noises, and any of a number of sleep interruptions. One of those contributors is overnight vital sign checks, generally present on standard admission order sets, done every 4 hours. The Choosing Wisely Campaign advocates to stop this reflex action, recommending the following1:
- Stop doing overnight vital sign checks for low-risk patients.
- Check overnight vitals for low-risk patients at 10p and 6a.
- Use pulse oximetry and regular nurse checks as a “balancing measure.”





Another suggestion is to use a scoring system to determine if a patient is at risk of catastrophic deterioration during an admission. A well-studied and validated system is the Modified Early Warning Score (MEWS).1 The table below, taken from Subbe et al, describes the scoring system. Patients with a score of 5 or greater were found in their prospective cohort study of 709 admissions to be associated with increased risk of death and
ICU admission.2
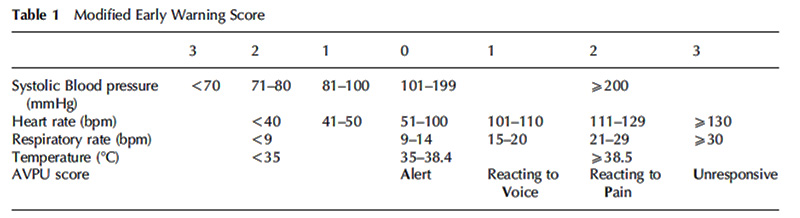
This system is very easy to use and consists of information already obtained during all admissions. It provides nursing staff with an additional tool that allows lower risk patients to sleep through the night, an important activity that promotes much needed healing. A small pilot study by Striver and colleagues compared two groups of patients staying overnight after a cardiac procedure, one group with standard every 4-hour vitals and the other left alone to sleep through the night. The group allowed to sleep reported less disruptive sleep and no escalation of care.3
With this information in mind, it appears safe to allow patients to sleep with a minimum of disruption. A rational approach to overnight vitals using an assessment tool to determine risk that empowers nurses to watch their patients “from afar” overnight has the potential to greatly improve the quality of hospital care for our recovering patients.
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]

-
Orlov NM, Arora VM. Routine Overnight Vital Sign Checks. J Hosp Med. 2020 May;15(5):272-274.
Follow this link -
Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. QJM. 2001 Oct;94(10):521-526.
Follow this link -
Stiver K, Sharma N, Geller K, Smith L, Stephens J, Daoud E, Moffat-Bruce S, Mazzaferri E. “Quiet at Night”: Reduced overnight vital sign monitoring linked to both safety and improvements in patients’ perception of hospital sleep quality. Patient Experience Journal. 2017;4(1):90-96.
Follow this link



















Comments
There are 0 comments for this article