

Practice Perfect 821
The Power of the Hand-held Doppler
The Power of the Hand-held Doppler


When I started podiatry school more than two decades ago, students in my class were given several instruments. At the time, they were foreign and exciting to see and touch (of course, everything at the time was novel). I had no clue at the time what most of them were for, and part of the excitement of my early podiatric clinical studies was learning when and how to use them. One of these instruments was a hand-held doppler ultrasound. It was pretty basic and didn’t print a report, but that didn’t matter. It added a powerful new weapon to battle those disorders of the foot and ankle. And, like the stethoscope, it incorporated the use of auditory input into the predominantly visual and tactile physical examination. I kept my doppler for many years until it finally died a few years ago. I quickly replaced this useful device.




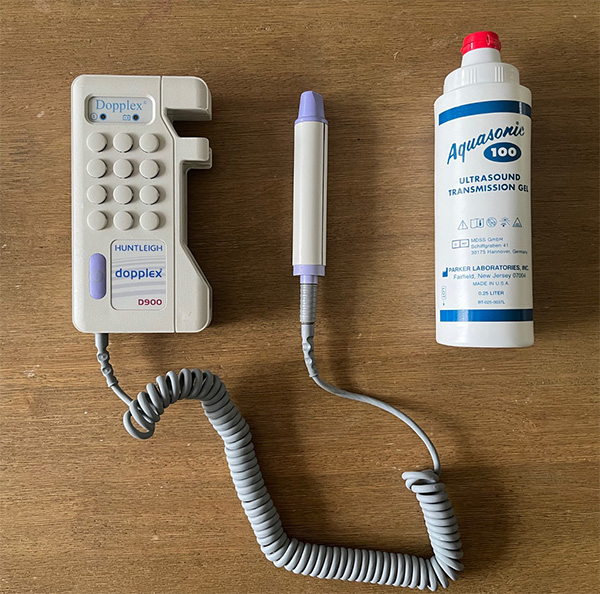
Over the years, especially as I became an educator of students and residents, I have found it odd how unmotivated my trainees are to use this device. They rely instead on pulse palpation as an almost sole physical examination finding to determine adequate blood supply to the foot. Research has shown that the physical examination, including pulse palpation and auscultation for femoral bruits has a high degree of accuracy (93.8%) compared with the ABI for peripheral arterial disease screening1. However, in clinical practice there are several pitfalls with pulse palpation that make this method less predictive. For example, the presence of obesity and edema make pulse palpation more difficult. The hand-held Doppler provides an excellent additional piece of information. With just a little practice, it is easy to use. Figure 1 shows the doppler I currently use.
It doesn’t take long to develop an ear for the tri-, bi-, or mono-phasic sounds typically heard in the lower extremity. Click on the audio files below to hear examples of a normal triphasic posterior tibial artery and an abnormal monophasic dorsalis pedis.
Audio file 1. Triphasic arterial flow (from the posterior tibial artery)
Audio file 2. Abnormal monophasic arterial flow (from the dorsalis pedis artery)
The hand-held doppler has other uses beside its application for simple pulse auscultation. Attinger and colleagues wrote an amazing comprehensive paper about the use of the angiosome concept in the foot and described an important set of examination techniques to determine if the flow to parts of the foot are by retrograde versus antegrade flow2. This article is long, detailed, and encyclopedic in its quality, and I can’t recommend an article more than this one. And in this milestone article, they use the hand-held doppler to determine the directionality of blood flow in the foot (see Figure 2 for a general demonstration of this method).
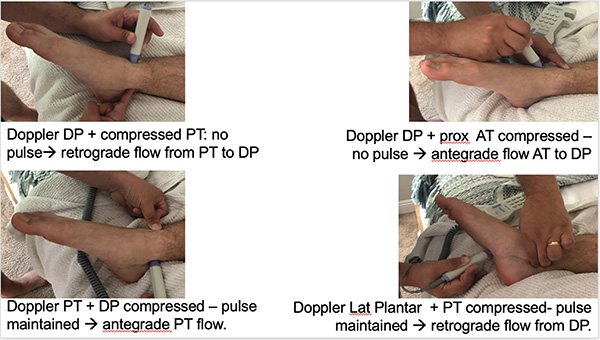
The importance of the concepts discussed in Dr Attinger’s manuscript is the clinical significance of retrograde and antegrade flow to the foot. It’s not just about “are the pulses palpable.” We can now be more nuanced in understanding the amount of perfusion to various parts of the foot. Keeping in mind that the first dorsal metatarsal artery is a major connection between the dorsal and plantar arteries, and that there are other anastamotic connections between the various major foot arteries, we can predict the viability of specific angiosomes if a particular artery or anastomosis is damaged. Table 1 shows the results of disruption of connections between the arteries of the foot if anastomoses are damaged depending on antegrade versus retrograde blood flow.
Table 1. Understanding flow to the foot in patients
with retrograde and antegrade blood flow.
| If anastomosis disrupted: | ||
| Dorsal flow | Plantar flow | Transmetatarsal amputation viability |
|
Antegrade DP |
Antegrade PT |
Both flaps OK. |
|
Antegrade DP |
Retrograde PT |
Plantar flap at risk. |
|
Retrograde DP |
Antegrade PT |
Dorsal flap at risk. |
Let’s discuss one more simple way to determine blood flow to the forefoot. In 2009, Haddock, et al published a paper describing the Lower-Extremity Allen Test (LEAT)3. This test is an adaption of the classic Allen test to determine dominant blood supply to the hand. See Table 2 below for a quick pictorial description of this test applied to the foot. One important application is for a vascular surgeon to determine to which artery to bypass during a revascularization or the main artery to open during an endovascular approach.
Table 2. The Lower-Extremity Allen Test explained.
| Explanation | Image | Interpretation |
|
Step 1: While dopplering the first dorsal metatarsal artery, occlude both the DP and PT arteries. |
 |
If sound remains, then perforating peroneal supplying collateral flow to the foot. |
|
Step 2: Keeping the doppler probe on the first dorsal metatarsal artery, allow flow back to the DP artery. |
 |
If sound remains, the DP is the primary artery to the foot. |
|
Step 3: Keeping the doppler probe on the first dorsal metatarsal artery, remove occlusion from both the DP and PT arteries. |
 |
If signal returns after release of the PT artery then this artery is the primary artery perfusing the forefoot. |
The hand-held doppler is a powerful technology, available at the point of care, to allow clinicians a better understanding of the blood supply to the foot. It really is the stethoscope of the foot.




Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]

-
Armstrong DW, Tobin C, Matangi MF. The accuracy of the physical examination for the detection of lower extremity peripheral arterial disease. Can J Cardiol. 2010 Dec;26(10):e346-350.
Follow this link -
Attinger CE, Evans KK, Bulan E, Blume P, Cooper P. Angiosomes of the foot and ankle and clinical implications for limb salvage: reconstruction, incisions, and revascularization. Plast Reconst Surg. 2006 Jun 1;117(7S):261S-93S.
Follow this link -
Haddock NT, Garfein ES, Saadeh PB, Levine JP. The lower-extremity Allen test. J Reconstr Microsurg. 2009 Sep;25(07):399-403.
Follow this link



















Comments
There are 0 comments for this article