

Practice Perfect 739
Sepsis, Steroids, and the Case of the Mysterious Leukocytosis
Sepsis, Steroids, and the Case of the Mysterious Leukocytosis

Let’s talk about a recent mystery I experienced. Let’s call it the Case of the Mysterious Leukocytosis. I was consulted on a 70-year-old diabetic male with a left foot infection (some details have been changed to maintain anonymity). On admission the patient was found to have a glycosylated hemoglobin of 11.1%, white cell count of 22,000, respirations of 23 breaths/minute, temperature 39 degrees Celsius, and blood pressure 80/40 mmHg. Radiographs showed gas in the plantar soft tissues (see the radiograph below), and he underwent emergent incision and drainage. Cultures later grew out Klebsiella ornitholytica, Staphylococcus aureus, Proteus mirabilis, and Enterococcus faecalis.
Figure 1. Radiographic appearance of the foot in question demonstrating gas in the plantar soft tissues.

The day after surgery the patient stated he “felt much better” and the postoperative wound appearance was greatly improved with viable remaining tissue. However, his leukocytosis elevated to a whopping 29,000 the next day. Here’s my mystery question for you: Why did the white blood count elevate after the successful surgery?
Here Are Some Choices to Consider:
A. This mixed infection causes worsening leukocytosis.
B. The patient is on steroids.
C. This represents post anesthesia cytokine release.
D. The uncontrolled blood sugar has falsely elevated the white blood cell count.
Well, Dr Sherlock Holmes, as you so astutely worked out, this patient must have septic shock and was on glucocorticoid steroids which caused the white blood cell count to elevate. One would expect the count to decline after a successful I&D (you’ll have to trust me that my surgery was successful). Although it is common to see a slight increase in the WBCs after surgery as a result of stress cytokines and hormones in response to anesthesia, this amount of elevation would not be expected. Option D simply does not happen. Although both WBCs and blood glucose simultaneously elevate in the presence of infection – highly common in diabetic patients – one does not cause the other.

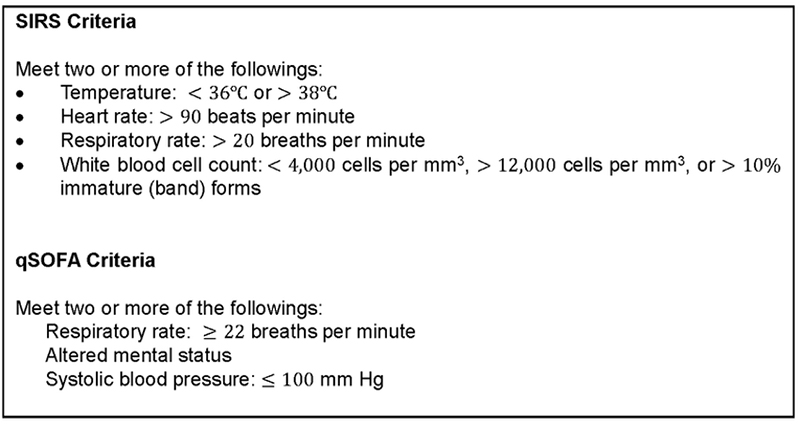
As it turns out, this patient had been started on hydrocortisone 50mg Q6H due to septic shock. Let’s discuss this a bit and focus on the high yield concepts. First, as a reminder, take a look at the table below that reminds us about the criteria for diagnosis of SIRS (Systemic Inflammatory Response Syndrome). In our patient’s case, he satisfied both SIRS and qSOFA criteria, and when you add to that the known source of infection, we have a diagnosis of sepsis.
Figure 2. Criteria for the diagnosis of SIRS and the use of the QSOFA score. Figure taken from Khojandi et al.1
But why the steroids - You ask?
This patient actually had septic shock and was started on hydrocortisone as part of the treatment. Obviously, the most important part of treatment for this was the incision and drainage to control the source of infection – yet another reason why podiatrists are so important – but let’s move on from there…

Septic Shock
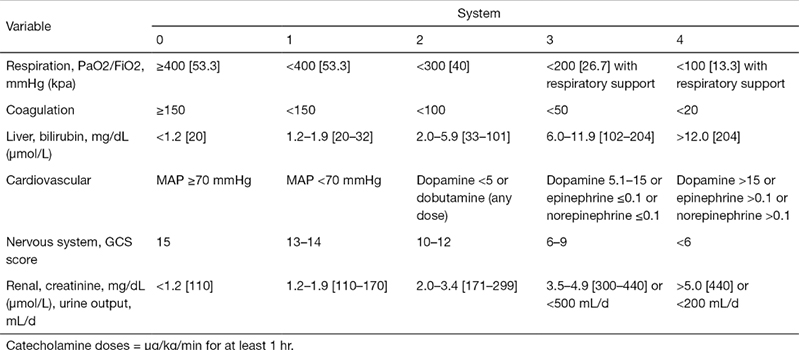
…And start with a definition of sepsis. According to the 2016 SCCM/ESICM task force, sepsis is defined as a “life-threatening organ dysfunction caused by a dysregulated host response to infection”.2 The Sepsis-3 guidelines (as these are termed) recommend using a SOFA score > 2 points as a diagnostic criterion because the SOFA score is for organ dysfunction rather than infection and is associated with an in-hospital mortality > 10%.2 For those interested in the full SOFA score, see Figure 3 at the end and the paper by Li et al3 where you’ll see why everyone likes to use the much shorter qSOFA score.
According to the Sepsis-3 criteria, then, septic shock is a subset of shock with “circulatory, cellular and metabolic abnormalities” with a greater mortality risk than sepsis alone (> 40%). The pathophysiology appears mostly related to uncontrolled vasodilation, and septic shock is diagnosed when these criteria are met: septic patients who require vasopressors to maintain a mean arterial pressure (MAP) > 65 mmHg despite adequate fluid resuscitation and have a lactate > 18mg/dL.2



But what about the steroids - You ask yet again?
Ok ok, I’m getting to it. Hold your horses! In septic shock, both the bacterial cell wall and endotoxins interact with the body to produce a systemic inflammatory response (hence the name, SIRS – smart, huh?). Cytokines such as tumor necrosis factor (TNA-alpha) and interleukin 1 (IL-1) are released which suppress adrenal responses to ACTH, decreasing systemic blood vessel tone, lowering blood pressure. Endotoxins additionally release nitric oxide synthase which also relaxes smooth muscle tone, lowering blood pressure further.4
Here's Why Steroids are Used
Corticosteroids reduce these effects, blunting the vasodilatory and hypotensive effects by preventing induction of nitric oxide synthase and enhance the response of blood vessels to catecholamines (norepinephrine and epinephrine)5, thus raising the blood pressure. Pretty snazzy drug, huh?

Dosing of Steroids in Septic Shock
Consensus guidelines recommend hydrocortisone 200-300mg/day IV (administered as 50mg Q6 hours) with a max of 400mg/day for at least 3 days and a taper thereafter to prevent rebound hypotension.6
The Final Piece of the Puzzle - Why the Excessive Leukocytosis?
And now – drum roll please – the final piece of our leukocytosis puzzle. We know that steroids cause an increase in blood glucose (via liver gluconeogenesis and decreased adipose glucose uptake) but why leukocytosis? Corticosteroids cause a decreased proportion of neutrophils that adhere to the vascular endothelium, releasing them into the blood, creating a neutrophilia and resulting leukocytosis. In fact, our mystery patient ran ~ 93% segmented neutrophils while on the steroids. This may have been related to the infection but likely was also attributable to the IV steroids. And there you have it fellow detectives. Case of the not-so-mysterious-leukocytosis solved. Until our next mystery…
Figure 3. Full SOFA scoring system for organ dysfunction. Chart taken from Li et al.


-
Khojandi A, Tansakul V, Li X, Koszalinski RS, Paiva W. Prediction of sepsis and in-hospital mortality using electronic health records. Methods Inf Med. 2018 Sep;57(04):185-193.
Follow this link -
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801-810.
Follow this link -
Li Y, Yan C, Gan Z, Xi X, Tan Z, Li J, Li G. Prognostic values of SOFA score, qSOFA score, and LODS score for patients with sepsis. Ann Palliat Med. 2020 May;9(3):1037-1044.
Follow this link -
de Kruif MD, Lemaire LC, Giebelen IA, van Zoelen MA, Pater JM, van den Pangaart PS, Groot AP, de Vos AF, Elliott PJ, Meijers JC, Levi M. Prednisolone dose-dependently influences inflammation and coagulation during human endotoxemia. J Immunol. 2007 Feb;178(3):1845-1851.
Follow this link -
Rees DD, Cellek S, Palmer RM, Moncada S. Dexamethasone prevents the induction by endotoxin of a nitric oxide synthase and the associated effects on vascular tone: an insight into endotoxin shock. Biochem Biophys Res Commun. 1990 Dec 14;173(2):541-547.
-
Annane, D., Pastores, S.M., Rochwerg, B. et al. Guidelines for the diagnosis and management of critical illness-related corticosteroid insufficiency (CIRCI) in critically ill patients (Part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Intensive Care Med (2017) 43:1751-1763. https://doi.org/10.1007/s00134-017-4919-5
Follow this link



















Comments
There are 0 comments for this article