
Practice Perfect 961
Journal Club: First MTP Joint Arthrodesis
Journal Club: First MTP Joint Arthrodesis


First metatarsophalangeal joint arthrodesis is an important fundamental procedure in the toolbox for podiatrists, so I’m always interested in seeing new research on this topic. In the March/April 2025 edition of the Journal of Foot and Ankle Surgery we see an interesting research study that lends further evidence toward a common issue: how much intermetatarsal angle (IMA) correction can we anticipate after a 1st MTP joint arthrodesis?
Understanding that this procedure closes an abnormal IMA is important, especially in those occasional cases where the surgeon has to consider closing a very large IMA first and then doing the 1st MTP joint fusion. Providing more information to help surgeons decide when to fuse alone or fuse after IMA correction will help us improve outcomes. Let’s do a quick journal club read-through.
Prediction of angular correction following first metatarsal-phalangeal joint arthrodesis1
Dr Meyr’s group out of Temple University performed their study to see if they could predict the amount of IMA before performing a first MTP joint arthrodesis (this had not been done previously in the literature). The researchers collected 2 years of radiographs on 18–90-year-old patients who underwent primary, isolated 1st MTPJ arthrodesis at one institution by 4 different surgeons. They measured the following angles using a computerized method: first IMA, hallux valgus angle, tibial sesamoid position, and hallux interphalangeus angle. Statistical calculations were performed to compare the preop and postop angles.
They reviewed 100 procedures with an average patient age of 62.04 +/- 8.60 years. To keep this focused, I’ll report only their first IMA and hallux abductus angle (HVA) results:
| Preop | Postop | |
| IMA | 11.65 +/- 4.23 | 10.01 +/- 3.60 |
| HVA | 25.94 +/- 14.44 | 15.01 +/- 8.55 |
*Both comparisons were found to have P < 0.001
After statistical analysis, they concluded that increased correction of the IMA could be expected with progressively larger pre-op IM angles, so the bigger the preop IMA the greater the correction, stating, “For every one degree of pre-operative IMA deformity over approximately 7 degrees, 0.38 degrees of correction might be expected.” They also found a relationship between the hallux valgus angle and IM angle, stating, “For every one degree of pre-operative HVA deformity over approximately 9 degrees, 0.63 degrees of correction might be expected.”
Looking at their data, a couple of issues come to mind. First, the average preoperative IMAs were low, and the average correction was also low. I’m used to seeing much larger IMAs in clinical practice and obtaining more correction than that. However, the range of IMAs was larger (7.42 to 15.88), and I wonder what the results would have looked like if patients with lower angles were excluded? This issue is the reason I reported their hallux abductus angles in the table. They did correct the hallux abductus angle by about 11 degrees average, but, again, I have to wonder what the IMA correction would have been if the surgeons had corrected that to an actual rectus position instead of abducted.



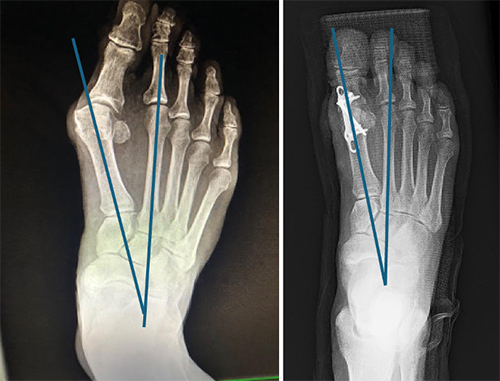
Let’s see if their predicted relationship works. Looking at Figure 1, you can see the DP weightbearing preop and postop radiographs of a patient of mine with HAV that underwent a 1st MTP joint arthrodesis. The preoperative IMA is 19 degrees (I’m hoping you can give me some leeway on the measurements – not easy on my computer!). According to this study, we should use 12 degrees (19 – 7 degrees) and the relationship would be 12 x 0.38 or 4.56 degrees of expected correction (for a predicted 14.44-degree postop IMA).
What did we actually get? I measured the postop IMA as 13 degrees (actual 6 degrees correction). That’s pretty close! The difference of 1.44 degrees between the predicted and actual would not have affected the clinical outcome. We should note that my postop hallux abductus angle is zero degrees (I usually aim to make this angle as close to zero as possible), which had more corrective power than if I had left some abduction.
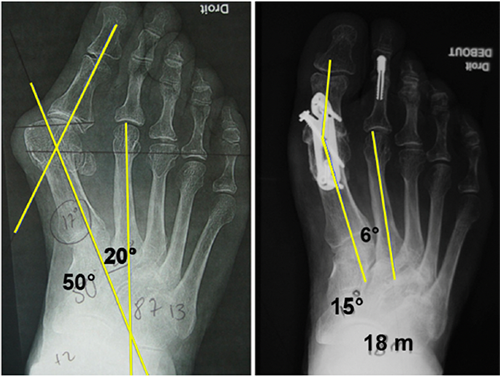
Let’s see a 2nd case to double check this. I pulled Figure 2 from a related research article by Dalat and colleagues2 who examined the same issue about to what extent 1st MTPJ fusions correcting the IMA. The figure shows a preop IMA of 15 degrees. According to Dr Myer’s prediction we should anticipate 3.04 degrees of correction and a 11.96-degree postop IMA. Dalat obtained an 8-degree IMA, much lower than predicted. What if we used the hallux abductus angle as described above? In the preop image it’s 40 degrees. So, using their relationship we would expect to see 31 x 0.63 = 19.53 degrees of correction or a postop IMA of -4.53 degrees. This one wasn’t close.
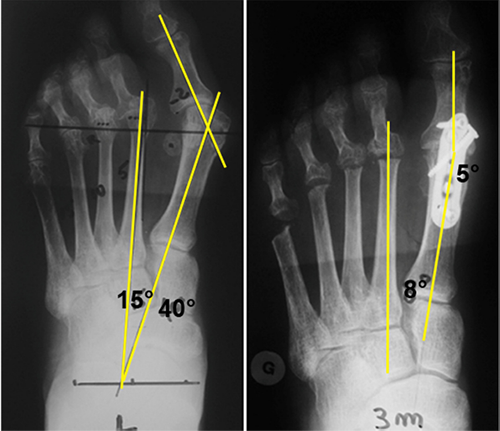
We need a tiebreaker, so let’s take one more case from Dalat’s study. Figure 3 shows a patient with a preop IMA of 20 degrees, which would be predicted to correct by 4.94 degrees or (20 -7) x 0.38 = 4.94 which would leave a predicted postop IMA of 15.06. This isn’t close to the 6 degrees they reported.
Despite these last two cases being different, I don’t think we should throw this relationship out. The major difference I see between case 1 and the other two is there were additional procedures performed. One of the exclusion criteria of the Myer study was adjunctive procedures. A pan metatarsal head resection, for example, has a lot more soft tissue dissection and looser tissue after removing the metatarsal heads and may affect the outcome.
With those thoughts in mind, we can say it’s well established that 1st MTP joint arthrodesis will close the first intermetatarsal angle, and now we may be able to predict the extent of closure. A validation study prospectively using these relationships would be a great next step. I’m sure we’ll continue to see a lot of excellent work from Dr Myer’s group as we have for many years.
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]

- Novoshelski S, Fazio S, Meyr AJ. Prediction of angular correction following first metatarsal-phalangeal joint arthrodesis. J Foot Ankle Surg. 2025 Mar-Apr;64(2):208-211.
Follow this link
- Dalat F, Cottalorda F, Fessy MH, Besse JL. Does arthrodesis of the first metatarsophalangeal joint correct the intermetatarsal M1M2 angle? Analysis of a continuous series of 208 arthrodeses fixed with plates. Orthop Traumatol Surg Res. 2015 Oct;101(6):709-714.
Follow this link
This blog and the overall sponsorship of PRESENT Podiatry was made possible through the support of our sponsors:
















Comments
There are 0 comments for this article