
Practice Perfect 943
Sodium Correction in Hyperglycemia
Sodium Correction in Hyperglycemia

It’s been a busy call week here in So Cal at the Chino Valley Medical Center residency, and I’ve been on the team with one of my first-year residents. As you might imagine, we’ve seen a number of patients with severe infections. At the beginning of our call week, my resident communicated to me that a couple of patients have hyponatremia. I asked why he kept telling me about that particular lab value (it wasn’t the only lab he communicated but seemed to be making a point to tell me).
“I was taught to watch sodium levels in patients with infections,” he said.
“Ok, then” I responded. “What’s the corrected sodium level?” He looked at me blankly.
Now, this resident is very sharp and knowledgeable having received an excellent medical education at his podiatric medical school, so I was a little surprised to experience his lack of knowledge on this point. If this good resident is missing some knowledge about hyponatremia in the face of hyperglycemia and infection, then it seemed like a good topic to discuss here.
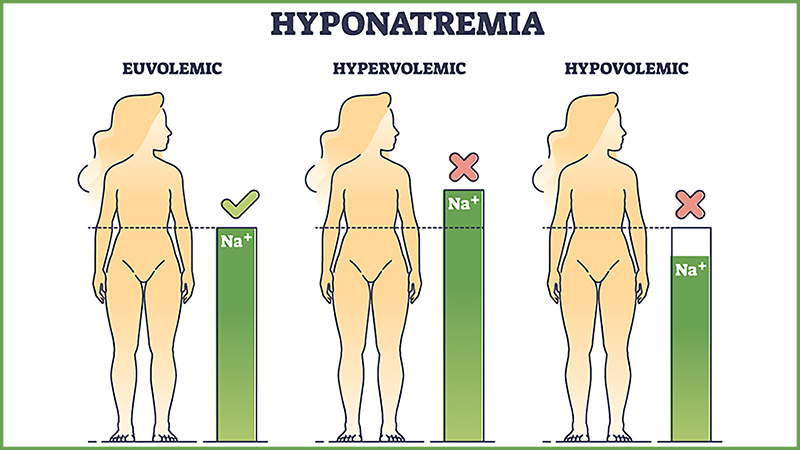
Hyperglycemia Leads to a Relative Hyponatremia
Consider that hyperglycemia is an excessive amount of glucose in the blood. This causes an osmotic shift of fluid from the intracellular space to the extracellular space. This extra fluid leads to a dilutional effect on sodium in the serum.
Calculating the Correction
Corrected NA+ = Measured Na+ 2.4((measured glucose – 100)/100)
Here’s a sample calculation:
We saw a 32-year-old diabetic patient admitted for a foot infection with sepsis. The measured sodium was 132 mEq/L and the measured glucose was 262 mg/dL.
Corrected Na+ = 132 + 2.4((262 – 100)/100)
Corrected Na+ = 132 + 2.4 (1.62)
Corrected Na+ = 136
Once corrected, this patient is not hyponatremic.



Why Is This Important?
From a general medical standpoint, it is important to correct the sodium level because one may mistakenly feel they need to intervene and treat the hyponatremia in a patient with elevated blood glucose. Similarly in patients with diabetic ketoacidosis or those with hyperosmolar hyperglycemic state, it’s important to understand the physiology when treating these conditions.
For the podiatrist, it’s important for the same reasons but also to consider hyponatremia in situations where sodium is considered a factor, like necrotizing fasciitis. As you’ll recall, the LRINEC score is used to predict the presence of this life-threatening infection (see Figure below). Note that sodium is one of the factors used.
Figure. LRINEC score. Taken directly from Wong, et al.1
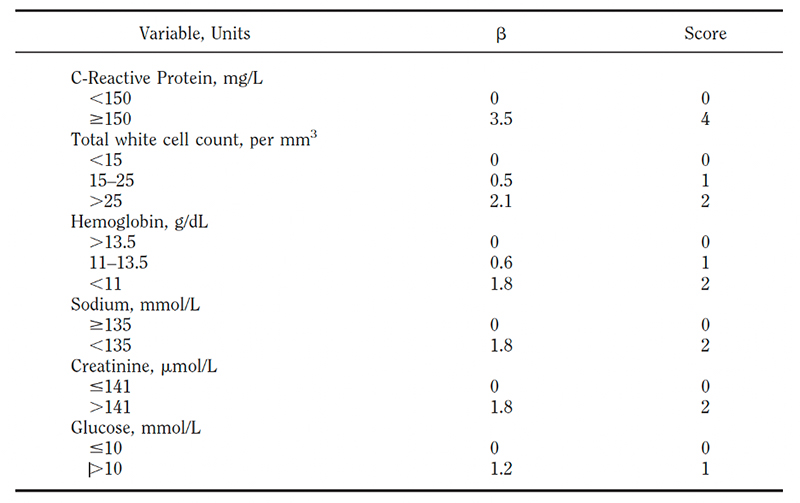
Since a score > 6 raises suspicion and a score > 8 is highly predictive of necrotizing fasciitis, the 0 or 2 either-or sodium score is likely to falsely elevate the LRINEC score in a patient with false hyponatremia in the presence of hyperglycemia.
This issue highlights the continued importance for podiatrists to understand the ever-increasing body of medical knowledge to maintain a global view of our patients rather than being simply foot doctors. Consider calculating the correction sodium in those patients with hyperglycemia.
Best wishes during your interviews!

Jarrod Shapiro, DPM, FACFAS, FACPM
PRESENT Practice Perfect Editor
[email protected]

Overall sponsorship of PRESENT Podiatry was made possible through
the support of our sponsors:















Comments
There are 1 comments for this article
Excellent article as always!