

PRESENT Podiatry is excited to announce a new resource for podiatric practice knowledge: Clinical Podiatry: A Best Practices Guide. This evidence-based clinical decision support resource is designed to help podiatrists make informed, point-of-care decisions when treating common foot and ankle conditions.
Over the next six months, a new guide will be published every week, each providing a concise 4-6 page review of a specific condition. These reviews will include expert opinions on best diagnostic and treatment practices, ensuring that you have the most up-to-date information at your fingertips. The series will cover a range of common conditions, including Onychomycosis, tinea pedis, plantar warts, and plantar fasciitis.
Each guide will be delivered directly to your email (unless you opt out) and will also be available on the PRESENT Podiatry website in the NEWS section, along with all past published blogs. To ensure the guides remain current, they will be reviewed and updated every few years. This approach mirrors the model of resources like UpToDate, allowing you to use these pieces as a reliable clinical reference, reading as little or as much of them as you need.
In addition to the written guides, each issue will be linked to a corresponding PRESENT On-Demand lecture on the topic. This provides an opportunity to dive deeper into the subject matter, learn more about the latest treatments and diagnostic techniques, and earn Continuing Medical Education (CME) credits.
The series is authored by Alex Fleischman, DPM, a resident in his first year at the New York College of Podiatric Medicine. The scholarly approach that he takes to this series ensures that the content is both relevant and grounded in current clinical practices, making Clinical Podiatry: A Best Practices Guide. an invaluable tool for enhancing your clinical practice and staying updated on the best practices in podiatry.
Onychomycosis

Introduction: Onychomycosis, derived from the Greek words “onyx” (nail) and “mykes” (fungus), refers to a fungal, yeast, or mold infection of the nail plate, nail matrix, and/or nail bed.1,2 Although onychomycosis can affect the fingernails and toenails, it is four to six times more prevalent in toenails because fungi, yeast, and mold favors the dark, warm, and moist environments provided by shoes.8
Patient Impact: Onychomycosis can cause physical damage to the soft tissue surrounding the nail, leading to pain and/or wound development. Additionally, patients may experience psychological distress due to the cosmetic disfigurement associated with fungal toenails.3,4
Clinical Outline:
- Presentation
- There are five subtypes of onychomycosis: distal lateral subungual onychomycosis (DLSO), white superficial onychomycosis (WSO), proximal subungual onychomycosis (PSO), endonyx onychomycosis, and candidal onychomycosis
- Diagnostics
- Common diagnostic tools for onychomycosis include KOH preparation, Periodic acid-Schiff (PAS)/Grocott’s Methenamine Silver (GMS) staining, fungal culture, Polymerase Chain Reaction (PCR) assays, and dermoscopy
- Treatment
- Treatment of onychomycosis includes oral antifungals, topical antifungals, nail debridement, and laser therapy
- Oral antifungals are of superior efficacy compared to topical antifungals
- Oral terbinafine is considered the gold standard treatment for onychomycosis based on clinical efficacy
- Topical antifungals should be used in mild case of onychomycosis, when patients are unable to tolerate oral treatment, or in combination with oral therapy
- Laser therapy is considered of similar efficacy to other treatments of onychomycosis
Expert Opinion from Warren Joseph, DPM, FIDSA:
On the diagnostic modalities…
The diagnosis of onychomycosis is highly physician dependent. Although as physicians, we often think we can visually diagnose onychomycosis with accuracy, confirmation is still necessary. Unfortunately, physicians typically do not have microscopes in their offices to perform sample analysis. Therefore, they send the samples out for results. This is why taking accurate nail samples is crucial. Moreover, the tests themselves are not always reliable, which reinforces the importance of proper nail collection to maximize the chances of an accurate microscopic analysis.
On the newer diagnostic modalities…
In addition to traditional methods, we should also expand our diagnostic skills into other areas, including dermoscopy. Sadly, only a few physicians use dermoscopy when analyzing onychomycosis or other dermatologic pathologies. Given that dermatologic pathologies are common in our offices, we should be more inclined to perform in-office analyses. It is a skill that we, as physicians, should improve upon to enhance care for our patients.
On the current diagnostic advances…
As physicians, we need to be more aware of the current research, particularly regarding PCR testing of fungal toenails. Literature suggests that some collected fungal nail specimens are resistant to terbinafine. In an article published in 2007, fungal nails that failed terbinafine treatment were PCR tested and revealed terbinafine resistance-conferring mutations in their SQLE gene. This finding reinforces the idea of conducting further testing prior to treatment to avoid overprescribing antifungals and to prevent the propagation of further antifungal resistance. Furthermore, it raises questions about the resistance of other fungal toenails to the available antifungal therapies.
On the definition of cure for onychomycosis…
It is very challenging to achieve the definition of a complete cure for onychomycosis. The definition of a cure for onychomycosis involves having a normal-looking nail and negative results from nail culture or microscopy. Unfortunately, even when the fungus is eradicated, the nail may still have other physical abnormalities unrelated to the infection. Furthermore, the diagnostic tests available to physicians are not the most reliable, which reinforces why the traditional definition of a cure is nearly unattainable.
Some of my colleagues and I have proposed a new definition of cure for onychomycosis. According to this definition, a cure is achieved if there is either a 100% absence of clinical signs of onychomycosis or negative mycological lab results, along with one or more of the following clinical signs: distal subungual onychomycosis affecting less than 10% of the nail plate, or nail plate thickening that does not improve with treatment due to co-morbid conditions. We encourage you to read this article to see how many of your patients might now be considered cured under this new definition.



Epidemiology: According to a 2024 meta-analysis of 108 studies, the overall prevalence of onychomycosis in the general population is approximately 4.0%.5 Additionally, onychomycosis presents in approximately 0.4% of children (under18 years old) and greater than 20% of the elderly (over 65 years old).6,7
Presentation: The physical characteristics of onychomycosis provide the physician with insights into the specific invading organism(s), the best treatment, and patient specific comorbidities. There are five subtypes of onychomycosis: distal lateral subungual onychomycosis (DLSO), white superficial onychomycosis (WSO), proximal subungual onychomycosis (PSO), endonyx onychomycosis, and candidal onychomycosis. Although each subtype has distinctive characteristics, they share common features including white or yellow-brown discoloration to the nail plate, subungual hyperkeratosis, onycholysis, and/or onychauxis.9
Distal lateral subungual onychomycosis (DLSO): This is the most common subtype of onychomycosis, accounting for 58%-85% of all cases.10 Pathologic development begins with fungal invasion of the hyponychium, followed by proximal progression of invasion through the nail plate.11 Typical presentation includes spiked channels splitting the nail plate and copious subungual debris.9,12 The most common invading organism of this subtype is Trichophyton rubrum.2
White superficial onychomycosis (WSO): This subtype accounts for approximately 10% of all cases of onychomycosis.2 Pathological development begins with loosely attached white patches of fungus on the dorsal aspect of the nail plate. If left untreated, fungi will continue to invade the remaining aspects of the nail unit. The most common invading organism of this subtype is Trichophyton mentagrophytes.11
Proximal subungual onychomycosis (PSO): This is the rarest subtype of onychomycosis. Pathogenesis begins with fungal invasion of the eponychium followed by distal progression of invasion through the nail plate.13 Typical presentation includes proximal onycholysis and leukonychia. The most common fungus associated with PSO is Trichophyton rubrum.14 Notably, this subtype is considered pathognomonic of patients with HIV infection by some physicians.15
Endonyxn onychomycosis: This subtype references when only the nail plate is invaded, rather than the entire nail unit. Organisms invade the nail plate without mounting an inflammatory response.16 Typical presentation includes a milky white texture and lamellar splitting to the nail plate. There is no onycholysis or subungual debris in this subtype.5 The most common fungi in endonyx onychomycosis is Trichophyton soudanense.11
Candidal onychomycosis: This subtype involves an infection of the entire nail plate with Candidal spp. Invasion occurs in areas of past trauma or fungal/bacterial infection.2 Typical presentation includes edematous and erythematous changes to the skin surrounding that nail plate and transverse depressions with convex changes to the nail plate. Unlike other subtypes, invasion begins in the soft tissue and spreads to the nail unit.14
Diagnostics: Diagnosis of onychomycosis is initially based on physical examination. However, several diagnostic modalities are recommended for confirmation. For proper pathologic analysis, a sample must be obtained from the area of highest concentration of infecting organisms. Such locations vary based on the subtype of presenting onychomycosis. Reference Figure 1 for information on proper specimen retrieval.
KOH preparation: A drop of 20% KOH is placed on a glass slide along with part of the collected sample for light microscopic analysis. The test is positive if hyphae, spores, and/or yeast are visualized.18 Based on a 12 study meta-analysis, the sensitivity and specificity of KOH preparation for onychomycosis was 61% and 95%, respectively.19
PAS/GMS staining: PAS is commonly part of the routine fungal microscopic analysis. In this stain, the glycogen and mucoprotein components of the cell wall of fungal hyphae are stained.20 Results take approximately 24 hours to return to the consulting physician.7 Based on a 12 study meta-analysis, the sensitivity and specificity of PAS stain for onychomycosis was 84% and 89%, respectively.19 GMS stains precipitate silver ions in polysaccharide walls of fungi ultimately producing a black stain under microscopy. Studies with high levels of evidence analyzing the sensitivity and specificity of the GMS stain for onychomycosis have not been conducted, but individual studies have reinforced that GMS stain and PAS stain are quantitatively similar in terms of sensitivity and specificity.
Fungal cultures: This method provide information about the type of infecting fungus, allowing for microbe specific antifungal therapy. Unfortunately, culture results can take days to weeks to yield results.9 Based on a 12 study meta-analysis, the sensitivity and specificity of fungal cultures for onychomycosis was 56% and 99%, respectively.19
PCR: This method compares sample genome sequences of onychomycosis to the genome sequence of a collected sample.21 Due to the cost and limit of availability to the physician, PCR testing is rarely used as a diagnostic tool for onychomycosis.22 Based on an institutional study, the sensitivity and specificity of PCR testing for onychomycosis was 80% and 62%, respectively.23
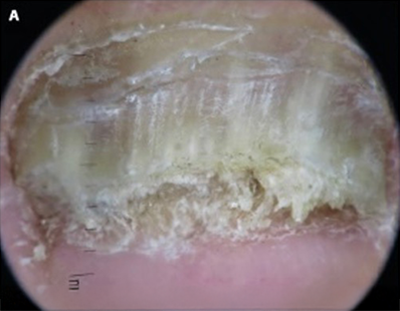
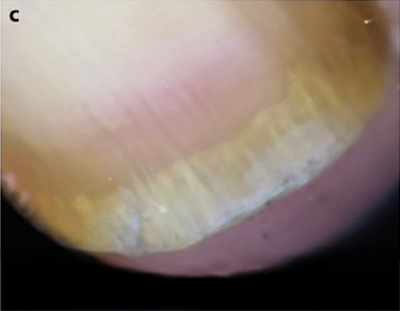
Dermoscopy of the nail (onychoscopy): This is a noninvasive hand-held method for bedside dermatologic evaluation of the nail. In a 2023 systemic review of 33 studies, the main dermatoscopic findings of onychomycosis were: subungual hyperkeratosis with distal irregular termination, longitudinal striae, and spikes. The sensitivity and specificity of subungual hyperkeratosis with distal irregular termination was 17.83% and 99.38%, respectively. The sensitivity and specificity of longitudinal striae was 39.79% and 83.78%, respectively. The sensitivity and specificity of spikes was 66.82% and 85.64%, respectively.25 It is important to note that dermoscopy is highly operator dependent, and therefore results may vary between physicians. Reference Figure 2 below for depictions of the dermatoscopic findings.
Treatment: Treatment options for onychomycosis include topical anti fungal therapy, oral antifungal therapy, and laser treatments.26,27
Oral antifungal therapy: A 2020 meta-analysis of 26 studies determined that oral antifungal therapy (terbinafine or itraconazole) is superior to topical antifungal therapy with respect to cure rates.28 A 2017 review of 48 studies found terbinafine to be the superior oral antifungal therapy based on cure rate.30 Consequently, terbinafine has become the gold standard treatment for onychomycosis.31
Topical antifungal therapy: This treatment is recommended for mild cases of onychomycosis or when oral antifungal therapies are contraindicated.28 Topical agents include ciclopirox, efinaconazole, and tavaborole. These agents are applied to the surface of the nail in hopes of penetrating the nail plate. Given the difficulty of penetration, physicians are advised to debride the nail plate or apply keratolytic agents (urea, salicylic acid, or lactic acid).17,26 Side effects of topical antifungals include exfoliation, erythema, and dermatitis.24
Laser therapy: A device emits wavelengths between 800 and 1400 nm that penetrate the nail, theoretically eliminating the invading organisms through a localized increase in temperature. Lasers act in pulsed dosages to prevent cosmetic nail deformations that would present with continuous use. Side effects include pain and bleeding.9,29 A 2024 meta-analysis comparing laser therapy to other treatment of onychomycosis showed similar efficacy compared to oral antifungal treatment.32
Conclusion: Onychomycosis is a condition associated with a fungal, yeast, or mold infection of the nail plate, nail matrix, and/or nail bed. There are five subtypes: distal lateral subungual onychomycosis (DLSO), white superficial onychomycosis (WSO), proximal subungual onychomycosis (PSO), endonyx onychomycosis, and candidal onychomycosis. Each subtype provides insight into specific invading organism(s), optimal treatment, and patient specific comorbidities. Onychomycosis can be diagnosed through physical exam and confirmed using KOH preparation, PAS stain, fungal culture, PCR or dermoscopy. Treatment options for onychomycosis include oral antifungal therapy, topical antifungal therapy and laser treatments, each with varying levels of success.

- Gelotar P, Vachhani S, Patel B, Makwana N. The prevalence of fungi in fingernail onychomycosis. J Clin Diagn Res. 2012 Dec 24;7(2):250-252. doi:10.7860/JCDR/2013/5257.2739
Follow this link
- Rodgers P, Bassler M. Treating onychomycosis [published correction appears in Am Fam Physician 2001 Feb 15;63(11):2129] Am Fam Physician. 2001;63(4):663-678.
Follow this link
- Gupta AK, Mays RR. The Impact of Onychomycosis on Quality of Life: A Systematic Review of the Available Literature. Skin Appendage Disord. 2018 Oct;4(4):208-216. doi:10.1159/000485632
Follow this link
- Frazier WT, Santiago-Delgado ZM, Stupka KC 2nd. Onychomycosis: Rapid Evidence Review. Am Fam Physician. 2021 Oct 1;104(4):359-367.
Follow this link
- Gupta AK, Wang T, Polla Ravi S, Mann A, Bamimore MA. Global prevalence of onychomycosis in general and special populations: An updated perspective. Mycoses. 2024 Apr;67(4):e13725. doi:10.1111/myc.13725
Follow this link
- Solís-Arias MP, García-Romero MT. Onychomycosis in children. A review. Int J Dermatol. 2017 Feb;56(2):123-130. doi:10.1111/ijd.13392
Follow this link
- Westerberg DP, Voyack MJ. Onychomycosis: Current trends in diagnosis and treatment. Am Fam Physician. 2013;88(11):762-770.
Follow this link
- Martin SM, Guffey DJ. The Youth Athlete. (Krabak BJ, Brooks A, eds.). Academic Press; 2023:187-201.
- Leung AKC, Lam JM, Leong KF, et al. Onychomycosis: An Updated Review. Recent Pat Inflamm Allergy Drug Discov. 2020;14(1):32-45. doi:10.2174/1872213X13666191026090713
Follow this link
- Mendoza N, Arora A, Arias CA, Hernandez CA, Madkam V. Clinical Mycology. 2nd ed. (Anaissie EJ, McGinnis MR, Pfaller MA, eds.). Churchill Livingstone; 2009:509-523.
- Grover C, Khurana A. Onychomycosis: newer insights in pathogenesis and diagnosis. Indian J Dermatol Venereol Leprol. 2012 May-Jun;78(3):263-270. doi:10.4103/0378-6323.95440
Follow this link
- Maskan Bermudez N, Rodríguez-Tamez G, Perez S, Tosti A. Onychomycosis: Old and New. J Fungi (Basel). 2023 May 12;9(5):559. Published 2023 May 12. doi:10.3390/jof9050559
Follow this link
- Lee KJ, Lee YB, Lee JY, Cho BK, Choi JS, Park HJ. Proximal Subungual Onychomycosis in a Patient with Classic Kaposi Sarcoma Caused by Trichophyton rubrum. Ann Dermatol. 2011 Sep;23 Suppl 1(Suppl 1):S11-S15. doi:10.5021/ad.2011.23.S1.S11
Follow this link
- Elewski BE. Onychomycosis: pathogenesis, diagnosis, and management. Clin Microbiol Rev. 1998 Jul;11(3):415-429. doi:10.1128/CMR.11.3.415
Follow this link
- Choudhary SV, Koley S, Mallick S, Bose S, Basak S. Proximal subungual onychomycosis caused by Aspergillus flavus in a HIV-positive patient. Indian J Dermatol Venereol Leprol. 2009 Jul-Aug;75(4):410-412. doi:10.4103/0378-6323.53152
Follow this link
- Bunyaratavej S, Bunyaratavej S, Muanprasart C, et al. Endonyx onychomycosis caused by Trichophyton tonsurans. Indian J Dermatol Venereol Leprol. 2015 Jul-Aug;81(4):390-392. doi:10.4103/0378-6323.157460
Follow this link
- Akhtar N, Sharma H, Pathak K. Onychomycosis: Potential of Nail Lacquers in Transungual Delivery of Antifungals. Scientifica (Cairo). 2016;2016:1387936. doi:10.1155/2016/1387936
Follow this link
- Ponka D, Baddar F. Microscopic potassium hydroxide preparation. Can Fam Physician. 2014 Jan;60(1):57.
Follow this link
- Velasquez-Agudelo V, Cardona-Arias JA. Meta-analysis of the utility of culture, biopsy, and direct KOH examination for the diagnosis of onychomycosis. BMC Infect Dis. 2017 Feb;17(1):166. Published 2017 Feb 22. doi:10.1186/s12879-017-2258-3
Follow this link
- Mahoney JM, Bennet J, Olsen B. The diagnosis of onychomycosis. Dermatologic Clinics. Vol 21. 3rd ed.; 2003 Jul:463-467.
- Yang S, Rothman RE. PCR-based diagnostics for infectious diseases: uses, limitations, and future applications in acute-care settings. Lancet Infect Dis. 2004 Jun;4(6):337-348. doi:10.1016/S1473-3099(04)01044-8
Follow this link
- Ghannoum M, Mukherjee P, Isham N, Markinson B, Rosso JD, Leal L. Examining the importance of laboratory and diagnostic testing when treating and diagnosing onychomycosis. Int J Dermatol. 2018 Feb;57(2):131-138. doi:10.1111/ijd.13690
Follow this link
- Navarro-Pérez D, García-Oreja S, Tardáguila-García A, León-Herce D, Álvaro-Afonso FJ, Lázaro-Martínez JL. Microbiological culture combined with PCR for the diagnosis of onychomycosis: Descriptive analysis of 121 patients. Mycoses. 2023 Dec;66(12):1045-1049. doi:10.1111/myc.13648
Follow this link
- Elewski BE, Aly R, Baldwin SL, et al. Efficacy and safety of tavaborole topical solution, 5%, a novel boron-based antifungal agent, for the treatment of toenail onychomycosis: Results from 2 randomized phase-III studies. J Am Acad Dermatol. 2015 Jul;73(1):62-69. doi:10.1016/j.jaad.2015.04.010
Follow this link
- Litaiem N, Mnif E, Zeglaoui F. N chomycosis: A Systematic Review. Dermatol Pract Concept. 2023 Jan 1;13(1):e2023072. Published 2023 Jan 1. doi:10.5826/dpc.1301a72L
Follow this link
- Malay DS, Yi S, Borowsky P, Downey MS, Mlodzienski AJ. Efficacy of debridement alone versus debridement combined with topical antifungal nail lacquer for the treatment of pedal onychomycosis: a randomized, controlled trial. J Foot Ankle Surg. 2009 May-Jun;48(3):294-308. doi:10.1053/j.jfas.2008.12.012
Follow this link
- Ma W, Si C, Kasyanju Carrero LM, et al. Laser treatment for onychomycosis: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Nov;98(48):e17948. doi:10.1097/MD.0000000000017948
Follow this link
- Gupta AK, Foley KA, Mays RR, Shear NH, Piguet V. Monotherapy for toenail onychomycosis: a systematic review and network meta-analysis. Br J Dermatol. 2020 Feb;182(2):287-299. doi:10.1111/bjd.18155
Follow this link
- Ma W, Si C, Kasyanju Carrero LM, et al. Laser treatment for onychomycosis: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Nov;98(48):e17948. doi:10.1097/MD.0000000000017948
Follow this link
- Kreijkamp-Kaspers S, Hawke K, Guo L, Kerin G, Bell-Syer SE, Magin P, Bell-Syer SV, van Driel ML. Oral antifungal medication for toenail onychomycosis. Cochrane Database Syst Rev. 2017 Jul 14;7(7):CD010031. doi: 10.1002/14651858.CD010031.pub2. PMID: 28707751; PMCID: PMC6483327.
Follow this link
- Kawa N, Lee KC, Anderson RR, Garibyan L. ONYCHOMYCOSIS: A Review of New and Emerging Topical and Device-based Treatments. J Clin Aesthet Dermatol. 2019 Oct;12(10):29-34
Follow this link
- Meretsky CR, Friday BL, Schiuma AT. Efficacy of Laser Therapy in Comparison With Other Methods for the Treatment of Onychomycosis: A Systematic Review and Meta-Analysis. Cureus. 2024 May 6;16(5):e59720. Published 2024 May 6. doi:10.7759/cureus.59720
Follow this link
Appendix
Figure 1
| Subtype | Methodology of Collection |
| DLSO | Use a sterile nail nipper to trim a full thickness section of the most proximal affected part of the nail plate as this area is of the highest concentration of invading organisms. Use a sterile curette to remove the underlying subungual debris for collection. |
| SWO | Use a sterile curette to remove the superficial debris from the nail plate for collection given that fungal colonization is localized to the dorsum of the nail plate |
| PSO | Use a sterile nail nipper to trim a full thickness sample of the most distal affected aspect of the nail plate as this area is of the highest concentration of invading organism. Use a sterile curette to remove the underlying subungual debris for collection |
| Endonyx | Use a sterile nail nipper to trim a full thickness sample with adequate visualization of the plantar aspect of the nail plate as this is the area of highest fungal concentration |
| Candidal | Use a sterile nail nipper to trim a full thickness portion of the lifted nail bed. Use a sterile curette to remove the underlying subungual debris for collection |
*Methodology referenced from resource (9) and physician recommendations
Figure 2

A: Ruin appearance
B: Longitudinal Striae
C: Spikes on proximal edge of onycholytic area
*Pictures supplied by resource (25)
Overall sponsorship of PRESENT Podiatry was made possible through
the support of our sponsors:

















Comments
There are 0 comments for this article