Welcome back to another Practice Perfect! For those of you who have hung with me for our ongoing series Making Practice Perfect Decisions, you’ll know that we concluded the series last week with Principle X. But, in the spirit of breaking rules, I couldn’t just end the series there. No, my friends, as I’ve mentioned both in this forum and in more lectures than I care to remember, making good decisions to benefit our patients is the single most important aspect of what we do. It then behooves me to throw in just one more editorial with a case example showing how these principles can be successfully used. With that said, let’s get to it!
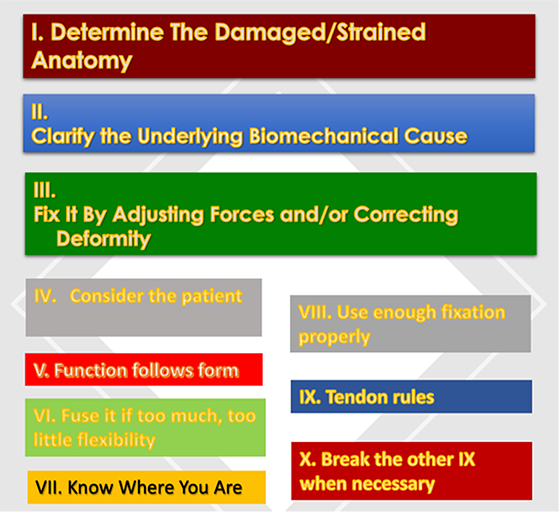
First, as a very quick refresher, take a look at Figure 1 below to recall the 10 principles of clinical decision-making. We’ll refer back to this figure as we discuss our case.
Figure 1. The ten principles of clinical decision-making.
Cyclical Topical Oxygen: Current Research and Clinical Evidence
Ron Guberman, DPM
Director of Podiatric Medical Education Co-Chief, Podiatry Division, Dept of Surgery Wyckoff Heights Medical Center Brooklyn, NY
Cyclical Topical Oxygen Therapy for wound healing continues to gain strong support in wound centers and with patients who utilize the therapy. Wound care professionals love seeing the positive results of this therapy and its use continues to grow as a result. There is also very strong research to support the use of this therapy that includes scientific research on oxygen usage and its benefits for wound healing as well as strong clinical evidence and Level I research that shows its advantages. Recent studies also show decreased hospitalizations and decreased amputations when using Cyclical Topical Oxygen Therapy. I will also share my own clinical experience with Cyclical Topical Oxygen Therapy that coincides with these results. I have found quite a few other advantages that I will share in my presentation.
Available Credits: CPME 0.5
The Case of Flat and Painful
A 56-year-old female complained of painful right medial arch that did not respond to shoegear changes, custom orthoses, physical therapy, and Richie bracing. It was time for surgery. Her past medical history was noncontributory except for a BMI of 35, placing her in the obese category. On physical examination, she had a highly flexible subtalar joint, unstable midtarsal joint and medial column (with supinatus of the forefoot), intact ankle joint, and painful posterior tibial tendon along its course and at the insertion on the navicular tuberosity. This yields a diagnosis of late stage 2 early stage 3 adult acquired flatfoot (or as the orthopedists are now calling it, progressive collapsing foot deformity). Her preoperative radiographs are shown in Figure 2. I have to apologize for the lack of clinical images and absence of the calcaneal axial and ankle radiographs. As time goes by, we sometimes lose pivotal images!
Figure 2. Preoperative radiographs demonstrating severe hindfoot pronatory collapse with > 50% talar head uncovering, a negative Meary’s angle, and decreased calcaneal inclination angle.
What surgical procedures would you chose for this patient? Before answering that, consider – especially after our completion of a series of articles about decision-making procedures – on what principles do you base your decisions? Do you choose based on what you were taught in residency? Or because doctor so-and-so told you to do so? I think we have to go beyond simple received wisdom and metacognitively consider logical reasons for the decisions we make. Hence, a 12-part series about decision-making principles!
Using the 10 principles as an analytic tool, I chose to do a double hindfoot fusion, Cotton midfoot osteotomy, and gastrocnemius recession. Table 1 splits out the reasoning, leading to this combination of procedures.
Table 1.
Principle
Application to Our Case
I. Determine the damaged/ strained anatomy.
PT tendon, spring ligament
II. Clarify the underlying biomechanical cause
Excessive peritalar instability, FF supinatus, calcaneal eversion, attenuated spring ligament
III. Fix it by adjusting forces and/or correcting deformity
Surgery (since nonsurgical methods failed)
IV. Consider the patient
Obese, fully ambulatory, expects to remain active with light walking
V. Function follows form.
VI. Fuse it if too much, too little flexibility
Realign forefoot and hindfoot all 3 planes (Meary’s, calc-tib angles talar head uncovering), excessive flexibility.
VII. Know where you are
Medial approach to the double hindfoot fusion with care to prevent damage to the deltoid ligament.
VIII. Use enough fixation properly
2 screw constructs for the TN and STJ fusions. No fixation needed for the Cotton procedure.
IX. Tendon rules
At the time, I performed a gastrocnemius recession. However, today I would not have done that procedure, since realigning the hindfoot would place the Achilles tendon medial to the STJ transverse axis, making it a supinator.
X. Break the other IX when necessary
Breaking the rules wasn’t needed in this case.
Figure 3. Postoperative appearance status post double hindfoot arthrodesis, Cotton osteotomy, and gastrocnemius recession.
I saw this patient several years after her recovery (to purchase a new pair of foot orthoses). Her pain was very much improved, and the repair was durable. Overall, she had a successful outcome. Consider the ten principles of clinical decision-making for your next case. You’ll find that a logical and thoughtful approach to your decisions will give you a foundation on which to not only choose treatments but also a way to analyze failures. In the end, it’s about making each of us better for the benefit of our patients.
Best wishes. Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor [email protected]
This ezine and the overall sponsorship of PRESENT Podiatry was made possible through the support of our sponsors: