Spindle Cell Hemangioma: A Case Report
Jay Lieberman,
DPM, FACFAS
with Steven D. Weiss, MD; Colette D’Altilio, DPM & Danielle Vonderlinden, DPM
| |
|
 Jay Lieberman,
Jay Lieberman,
DPM, FACFAS
|
Abstract: A 45-year-old white male presented with multiple nodules on the right lower extremity.
The lesions had been present for many years and recently one nodule had become painful. This nodule was removed and pathological evaluation initially gave the diagnosis of a hemangioma. Postoperatively, the patient developed multiple new nodules in this same area. Subsequent excisional biopsy and microscopic examination demonstrated a histological appearance consistent with spindle cell hemangioma (SCH). Spindle cell hemangiomas are benign lesions once termed hemangioendothelioma because of its “field effect recurrences” which was speculated to be metastasis. First described in 1986 by Weiss and Enzinger, SCH, has a distinct histological appearance and biologic behavior. This unusual lesion has been mistaken for Kaposi’s sarcoma, angiosarcoma and cavernous hemangioma.
|
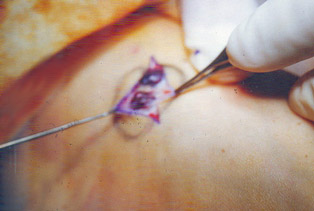
Figure 2. Post Biopsy � Lesion along
DIPJ and PIPJ removed |
|
Spindle Cell Hemangioma: A Case Report:
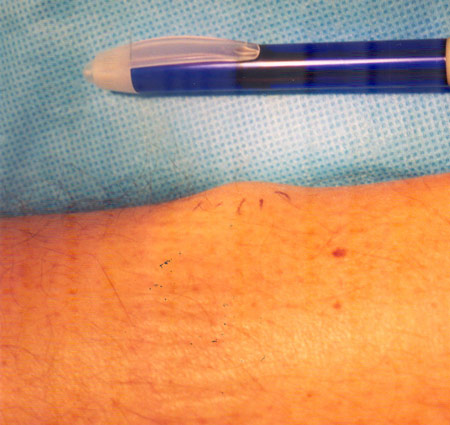
A 45-year-old homosexual male in a monogamous long-term relationship complained about multiple bluish nodules on his right leg and foot, occasionally grouped together. These globular lesions measured 0.5-2 cm in diameter and occurred over the proximal medial interphalangeal joint and the distal interphalangeal joint, of the third toe, as well as across the dorsal midtarsal foot and the Achilles tendon area.
The two lesions on the toe had become painful especially when ambulating in closed shoe gear. These nodules appeared to be freely moveable under the skin, cystic in nature and collapsed with limb elevation. The lesions were present in excess of three years. There is no family history of any similar type of lesions. The patient’s CBC and Chem 7 were unremarkable. A recent HIV test was negative. On physical examination, there was no evidence of lymphadenopathy, organomegally or masses and no other dermatologic conditions were noted.
An excisional biopsy was performed on the symptomatic lesions of the third pedal digit. Pathologic studies initially reported a diagnosis of hemangioma. Postoperatively, the patient developed additional lesions along the posterior leg with the previously asymptomatic nodules now becoming painful and increasing in size.
|
|
Figures 3: SubtalarJoint |
Figures 4: Gastroc Preop |
|
|
|
Figures 5: Subtalar Joint Intraop smaller |
Figures 6: Gastroc Intraop |
|
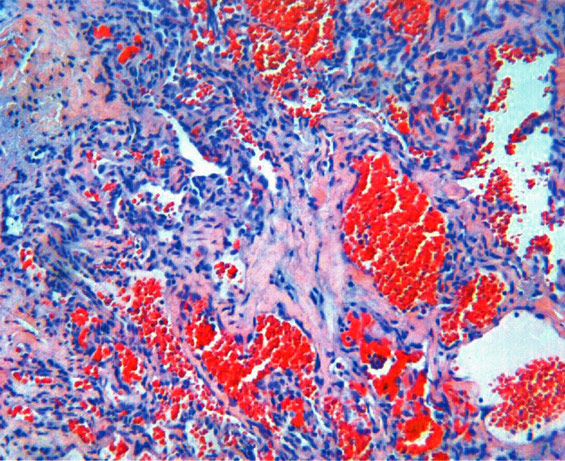
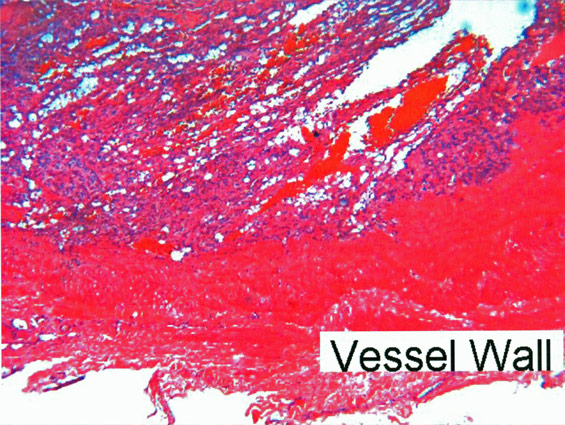
Histologic Findings:
|
Figures 9: Gastroc Intraop |
|
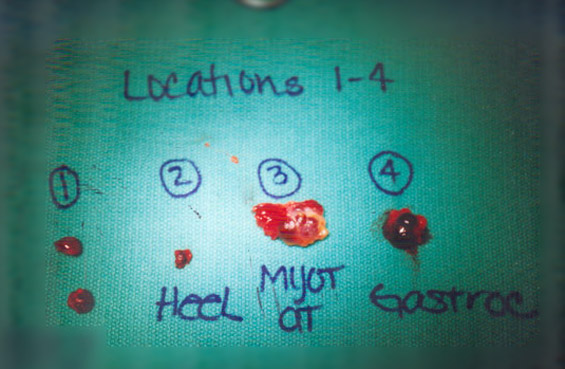
Pathologic examination revealed findings typical of SCH. The features of both the most recent and previous excisions were similar. Grossly, the lesions were well circumscribed. Microscopic examination showed multiple vascular channels of varying caliber. The channels were lined by a layer of endothelial cells. The intervening stroma contained numerous plump spindle cells similar in appearance to the endothelial cells. Some of the vascular spaces were engorged with blood. Several contained thrombi.
Discussion:
Historically, SCH, first described by Weiss and Enzinger, was thought to be a low-grade form of angiosarcoma with frequent recurrences. The lesion was originally given the designation of Spindle Cell Hemangioendothelioma. Further evaluation of the original studies have found the lesion to be benign.
The tendency of SCH to recur led to the initial belief that this was a low-grade sarcoma. Perkins and Weiss, however, reevaluated their original study. It was determined that no metastases had occurred in any individual case. The recurrences appeared in fact to represent a “field effect” of this lesion: a predisposition to develop additional lesions in a zonal distribution, independent of whether earlier lesions are excised. The fact that the recurrences only appeared in the region of the original lesion gave evidence that these were not true metastases.
SCH is a benign vascular lesion, which is usually superficial and has a dark appearance. Over a third of these lesions will occur on the foot. Often found in groups, the individual lesions usually measure up to 2.0 centimeters in diameter and are found most commonly in the dermis and subcutaneous tissue. Males and females are equally affected at any age. The highest incidence is in childhood and early adulthood. Fifty percent involve a large preexisting vein or artery. Local recurrences occur in the same general area. SCH has been associated with Marfucci’s Syndrome, Klippel-Traunay syndrome, and lymphedema, all of which may contribute to a compromise in a blood flow to the area. One study reveals that 5% of patients with SCH had concomitant Marfucci’s syndrome (evident by the presence of multiple enchondromas with almost half of these lesions present on the distal lower extremities). This indicates that these groups of disorders may be especially relevant to the podiatric profession.
Its pathogenesis has been disputed as long as it has been recognized. Some authors speculate that SCH is a reaction to thrombosis and organization while most others suggest that there is an underlying vascular abnormality. Once the benign nature of this disorder is understood, distinguishing a vascular malformation from a true neoplasm may be arbitrary.
An important differential diagnosis of this lesion is Kaposi’s sarcoma (KS). The appearance of SCH and KS is similar on gross examination with a purple hue and an early ability to blanch. Histological evaluation of each reveals a spindle cell proliferation with antler like vascular channels. However, SCH is rarely intravascular and lacks cavernous spaces or vacuolated endothelial cells.
No significant interruption of function has been reported. Most patients’ concern is mainly cosmetic, although with more than one third of these lesions occurring on the feet, pain within closed shoe gear and pain on ambulation can be expected. Conservative treatment is therefore recommended. Single or multiple lesions may be treated with local excision.
References:
- P. Perkins and S. W. Weiss, “Spindle cell hemangioendothelioma: an analysis of 78 cases with reassessment of its pathogenesis and biologic behavior,” American Journal of Surgical Pathology, vol. 20, no. 10, pp. 1196–1204, 1996.
- Tomasini C, Aloi F, Soro E, Elia V: Spindle Cell Hemangioma. Dermatology 1999;199:274-276
- Nayler SJ, Rubin BP, Calonje E, Chan JKC, Fletcher CDM: Composite Hemangioendothelioma: a complex, low grade vascular lesion mimicking angiosarcoma. Am J Surg Pathol, 24: 352-361, 2000.
- Guillou L, Fletcher CD: Benign lymphangioendothelioma (acquired progressive lymphangioma): a lesion not to be confused with well-differentiated angiosarcoma and patch stage Kaposi's sarcoma: clinicopathologic analysis of a series. Am J Surg Pathol 2000, 24:1047-1057.
- Enzinger FM, Weiss SW Soft tissue tumours, 2nd ed 1988: pp489, 538-42, 573
- Kempson R L, Fletcher C D M, Evans H, Hendrickson M R, Sibley R K. Tumors of the soft tissues. Atlas of Tumor Pathology.. pp 310,332-34.
Get a steady stream of all the NEW PRESENT Podiatry
eLearning by becoming our Facebook Fan.
Effective eLearning and a Colleague Network await you. |
 |