Functional Foot Type Closed Chain Characteristics
|
|
By Dennis Shavelson, DPM
Biomechanics Editor, PRESENT Podiatry |
As discussed foundationally, each Functional Foot Type(FFT) has a set of characteristics associated with that foot type1-2-3.
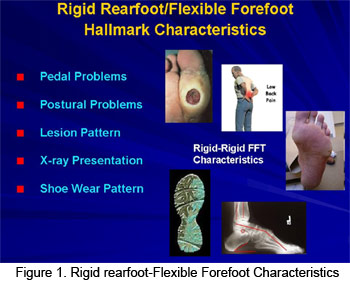 Although some of the characteristics may be shared by more than one foot type, there are some (or a group of some), for each of the FFT’s, that characterize that foot type. The more characteristics of a foot type present in a given patient, the closer that patient is to being a “pure” example of that foot type3. (See figure 1) Although some of the characteristics may be shared by more than one foot type, there are some (or a group of some), for each of the FFT’s, that characterize that foot type. The more characteristics of a foot type present in a given patient, the closer that patient is to being a “pure” example of that foot type3. (See figure 1)
This means that beyond the SERM-PERM testing4 for a patient’s FFT, overlaps can be determined which impact the clinical care decisions of patients by analyzing the presenting characteristics of each patient as a starting point to developing a plan for foot type-specific care.
In addition, as previously discussed, there are concomitant factors, such as weight, activity level, health state, etc. that impact the extent and progression of hallmark characteristics.
Although many patients share the same foot type, variations in closed chain characteristics and concomitant factors make each patient a case of one and well trained and practiced Functional Foot Typers dispensing Foot Centrings are once again finding themselves atop the biomechanical pyramid that Dr. Root placed us on thirty + years ago.
Hallmark Foot Typing Characteristics
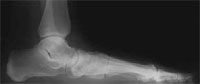
X-Ray Presentation
| FFT |
X-ray Characteristics |
| Rigid/Rigid |

| High CIA++++, Bullet Hole Sinus Tarsi ++++, Intact CYMA Line ++++, Low Talo Calc Angle ++++, Lateral STJ Axis ++++, Plantarflexed 1st Ray ++++, Low HAV++++, Low IM++++, Low PASA++++ |
|
| Rigid/Stable |
High CIA+++, Bullet Hole Sinus Tarsi +++, Intact CYMA Line ++++, Low Talo Calc Angle +++, Lateral STJ Axis +++, Plantarflexed 1st Ray +++, Low HAV+++, Low IM+++, Low PASA+++ |
| Rigid/Flexible |

| High CIA+++, Bullet Hole Sinus Tarsi +++, Intact CYMA Line ++++, Low Talo Calc Angle +++, Lateral STJ Axis +++, Plantarflexed 1st Ray +++, Low HAV+++, Low IM+++, Low PASA+++ |
|
| Rigid/Flat |
High CIA++, Bullet Hole Sinus Tarsi ++, Intact CYMA Line ++, Low Talo Calc Angle ++, Lateral STJ Axis ++, Plantarflexed+ or Dorsiflexed+-++++ 1st Ray, HAV +-++++, IM +-++++, PASA, +-++++, |
| Stable/Stable |

| Normal CIA, Sinus Tarsi, CYMA Line, Talo Calc Angle, Neutral STJ Axis, Neutral 1st Ray, Normal HAV, IM and PASA |
|
| Stable/Flexible |
Low CIA+, Closed Sinus Tarsi+, Broken CYMA Line+, High Talo Calc Angle+, Lateral STJ Axis+, Dorsiflexed 1st Ray+, High HAV+, High IM+ and High PASA+ |
| Stable/Flat |
Low CIA++, Closed Sinus Tarsi++, Broken CYMA Line++, High Talo Calc Angle++, Lateral STJ Axis++, Dorsiflexed 1st Ray++, High HAV++, High IM++, High PASA++ |
| Flexible/Flexible |
| Low CIA+++, Closed Sinus Tarsi+++, Broken CYMA Line+++, High Talo Calc Angle+++, Lateral STJ Axis+++, Dorsiflexed 1st Ray+++, High HAV+++, High IM+++, High PASA+++ |
|
| Flexible/Flat |
Low CIA++++, Closed Sinus Tarsi++++, Broken CYMA Line++++, High Talo Calc Angle++++, Lateral STJ Axis++++, Dorsiflexed 1st Ray++++, High HAV++++, High IM++++, High PASA++++ |
| Flat/Flexible |
Vertical CIA, Obliterated Sinus Tarsi, Broken CYMA Line++++, High Talo Calc Angle++++, Lateral STJ Axis++++, Dorsiflexed 1st Ray++++, High HAV++++, High IM++++, High PASA++++, Arthritic Changes Rearfoot and Forefoot++ |
| Flat/Flat |

| Vertical-Negative CIA, Obliterated Sinus Tarsi, Fixed and Broken CYMA Line++++, High Talo Calc Angle++++, Lateral STJ Axis++++, Dorsiflexed 1st Ray++++, High HAV++++, High IM++++, High PASA++++, Advanced Arthritic Changes Rearfoot and Forefoot++ |
|
Pedal Conditions
| FFT |
Foot Conditions |
| Rigid/Rigid |
Hallux Rigidus +++, Hallux Malleus, 1=5 Hammertoes, Haglund’s Deformity++++ |
| Rigid/Stable |
Bunions+, FHL ++, FHE +, 2-5 Hammertoes + |
| Rigid/Flexible |
Bunions+-++++, FHL +-++++, FHE, +-++++, 2-5 Hammertoes +-++++, Plantar Fascitis +++, Morton’s Neuroma +++, Met Cuneiform Exostosis +++, Bunionette +++ |
| Rigid/Flat |
Bunions++++, FHL ++++, 2-5 Hammertoes ++++ |
| Stable/Stable |
Problems only if patient is overweight, overactive, bunions + late, Plantar Fasciitis +, Bunionette ++ |
| Stable/Flexible |
Bunions ++, FHL ++, FHE ++, 2-5 Hammertoes, Morton’s Neuroma ++, Met Cuneiform Exostosis ++ |
| Stable/Flat |
Extremely Rare Foot Type, Surgical Failure, i.e. met primus elevatus postop |
| Flexible/Flexible |
PTTD +++, Bunions Late+-++++, Extensor Substitution +-++++ |
| Flexible/Flat |
PTTD ++++ |
| Flat/Flexible |
Extremely Rare Foot Type, Surgical failure i.e. valgus producing dwyer postop, PTTD + |
| Flat/Flat |
Non Functional, Non Correctable Foot Type, Surgical Salvage Considerations, Low Level Lifestyle |
| Flat/Flat |
Non Functional, Non Correctable Foot Type, Surgical Salvage Considerations, Low Level Lifestyle |
| General Guidlines |
Rearfoot Alone |
Forefoot Alone |
| Rigid |
Poor Shock Absorption, Poor Morpher, Excellent Rigid Lever |
Hallux Rigidus, 1-5 Hammertoes, |
| Stable |
Good Shock Absorber, Good Morpher, Good Rigid Lever |
Bunion, 2-5 Hammertoe, Plantar Fascial and Neuroma Problems Late and Low Level |
| Flexible |
Excellent Shock Absorber, Excellent Morpher, Poor Rigid Lever |
Bunions, 2-5 Hammertoes, Neuromata, Bunionette, Plantar Fascitis, 2nd Met Capsulitis, Freibergs, 2nd Met Stress Fracture |
| Flat |
Poor Shock Absorber, Poor Morpher, Poor Rigid lever |
NON Functional, Osteoarthritis +++ |
Postural Sequellae
| FFT |
Postural Information |
| Rigid/Rigid |
Equinus +++, Shock problems, degenerative knee, hip, lower back problems, tight musculature |
| Rigid/Stable |
Equinus ++, Shock problems |
| Rigid/Flexible |
Equinus ++, Knee, Lower back Problems Early, Runners Knee, Shin Splints |
| Rigid/Flat |
Equinus +, Severe Postural Sequelae, Low Back, Knees, Hips |
| Stable/Stable |
No Postural Sequelae Unless Stressed or Overused |
| Stable/Flexible |
Collapsed Posture, Knee Hip, Low Back Sequelae |
| Stable/Flat |
Severe Postrual Sequelae, Late |
| Flexible/Flexible |
Genu Valgum, Coxa Vara, Lumbar Lordosis, Shin Splints, Runner’s Knee, Collapsed Posture Early, Poor Function |
| Flexible/Flat |
Genu Valgum, Coxa Vara, Lumbar Lordosis, Shin Splints, Runner’s Knee |
| Flat/Flexible |
Poor Performance |
| Flat/Flat |
Very Poor Performance, Major Postural Sequelae included, Gait |
| FFT |
Rearfoot Alone |
Forefoot Alone |
| Rigid |
Postural Shock Problems, Equinus, Degenerative Joint Disease |
Shock Problems, Degenerative Joint Disease |
| Stable |
Stable Posture Unless Stressed |
Depends on Rearfoot |
| Flexible |
Flexible Posture, Collapse +++ |
Depends on Rearfoot |
| Flat |
Tight, Non Functional Posture |
|
Characteristic Lesion Patterns
| FFT |
Lesion Patterns |
| Rigid/Rigid |
First Met Callus |
| Rigid/Stable |
Mild First Met or Second Met Callus |
| Rigid/Flexible |
Medial Heel Callus ++, IP Hallux Callus +++, 2nd Met callus |
| Rigid/Flat |
5th Met Callus ++ |
| Stable/Stable |
Callus Hallux IP Joint, 2nd Met If Stressed or Late |
| Stable/Flexible |
Medial Heel Callus + |
| Stable/Flat |
Medial Heel Callus + |
| Flexible/Flexible |
Medial Heel Callus+++, Medial First Met Callus ++, IP Hallux Callus ++, 2nd met callus+++, 5th Met callus++ |
| Flexible/Flat |
Medial Heel Callus, Medial First Met Callus +++, IP Hallux Callus ++, 2nd met callus++++, 5th Met callus+++ |
| Flat/Flexible |
Fifth Met Callus +++= |
| Flat/Flat |
Fifth met Callus ++++ |
| FFT |
Rearfoot Alone |
Forefoot Alone |
| Rigid |
Callus Depends on Forefoot |
First met Callus |
| Stable |
Callus Depends on Forefoot |
|
Mild or Late 2nd met callus, Mild 5th met Callus, Mild IP Hallux Callus |
| Flexible |
Navicular Callus |
2nd met Callus, IP Hallus Callus, 5th met Callus |
| Flat |
Lateral heel callus, Fifth Met Callus |
5th Met Callus |
Shoe Wear Characteristic
| FFT |
Lesion Patterns |
| Rigid/Rigid |
Medial Heel Wear ++++, 1st met Wear+++, 5th met Wear+ |
| Rigid/Stable |
Medial Heel Wear ++++ 1-2 Met Wear, 5th Met Wear++ |
| Rigid/Flexible |
Medial Heel Wear ++++, Lateral Forefoot Wear, 2nd met Wear ++, IP Hallux Wear +++ |
| Rigid/Flat |
Medial Heel Wear ++++, 5th Met ++++ |
| Stable/Stable |
Medial Heel Wear ++, Normal Forefoot Wear Unless Stressed |
| Stable/Flexible |
Medial Heel Wear ++ |
| Stable/Flat |
Medial Heel Wear ++, 5th met Wear ++ |
| Flexible/Flexible |
Medial Heel Wear +, Expanded Medial Counter +++ |
| Flexible/Flat |
Medial Heel Wear +, Expanded Medial Counter ++++ |
| Flat/Flexible |
Lateral Heel Wear ++, Lateral Forefoot Wear ++++ |
| Flat/Flat |
Lateral Heel Wear +++, Lateral Forefoot Wear ++ |
| FFT |
Rearfoot Alone |
Forefoot Alone |
| Rigid |
Narrow Forefooted Shoe, Medial Heel Wear ++++, Needs High Throat |
First Met Wear, Fifth Met Wear |
| Stable |
|
2-3 Met Wear |
| Flexible |
Wide Forefooted ShoeMedial Heel Wear +, Medial Midsole Wear, Medial Counter Expanded |
2nd Met,Wear, Fifth Met Wear, IP Hallux Wear |
| Flat |
Wide Forefooted Shoe, Lateral Heel Wear, Needs Low Counter |
Lateral Forefoot Wear |
FFT Precursors
| FFT |
Precursors |
| Rigid/Rigid |
Sinus Tarsi, MP Flexion ++++, Medial Calcaneal ++, Cuboid |
| Rigid/Stable |
Sinus Tarsi ++, MP Flexion ++, Medial calcaneal ++ |
| Rigid/Flexible |
Sinus Tarsi ++MP Flexion +++, 2nd Met +++, Medial Calcaneal +++ |
| Rigid/Flat |
Sinus Tarsi ++++MP Flexion ++, Medial Calcaneal +++ |
| Stable/Stable |
Precursors When Stressed or Late |
| Stable/Flexible |
MP Flexion +++, 2nd Met ++ |
| Stable/Flat |
Sinus Tarsi +, 2nd met + |
| Flexible/Flexible |
PTTD, 2nd met ++, Medial Calcaneal |
| Flexible/Flat |
PTTD, |
| Flat/Flexible |
PTTD, |
| Flat/Flat |
Sinus Tarsi, Navicular, Cuboid |
| FFT |
Rearfoot Alone |
Forefoot Alone |
| Rigid |
Sinus Tarsi |
MP Flexion, 1st Met, 1st Met Cuneiform |
| Stable |
Precursors When Stressed or Late |
None Unless Stressed or Overused |
| Flexible |
PTTD, Cuboid, 5th Met Base |
MP Flexion, 2nd met, 5th Met head |
| Flat |
PTTD, Cuboid, 5th Met Base |
2nd met, 5th Met, Navicular, Cuboid |
| Legend |
Depending on Confirmatories and Purity of FFT |
| + |
Mild and/or Late Development |
| ++ |
Moderate and/or Earlier Development |
| +++ |
Major and Early Development |
| ++++ |
Major and Late Development |
References:
- Shavelson, Dennis: The Pedal Snowflakes, The Foot in Closed Chain, Present Podiatry Ezine 09/14/09: https://www.podiatry.com/ezines/?pub_year=2009§ion_id=51#ezine509
- Shavelon, Dennis: A Closer Look at Neoteric Biomechanics; Podiatry Today, September 2007, pp 147-153
- Shavelson, D. Steinberg,J, Bakotic, B: Chapter 25, The Diabetic Foot;Principles of Diabetes Mellitus, 2nd Edition, Elisiver Publishing, Switzerland; February, 2010 pp 528-551
- Shavelson, Dennis: The Functional Foot Typing Forefoot Examination; The Foot In Closed Chain, Present Podiatry; Ezine 03/29/10:
https://www.podiatry.com/ezines/?pub_year=2010§ion_id=51#ezine584
|
|

































